

Pacemaker lead rupture in a patient with subacute endocarditis: a case report
- PMID: 35174311
- PMCID: PMC8843865
- DOI: 10.1093/ehjcr/ytac054
Pacemaker lead rupture in a patient with subacute endocarditis: a case report
Abstract
Background: Cardiac implantable electronic device (CIED)-related infections are associated with severe morbidity and mortality. Few cases have previously documented both lead endocarditis and lead rupture simultaneously.
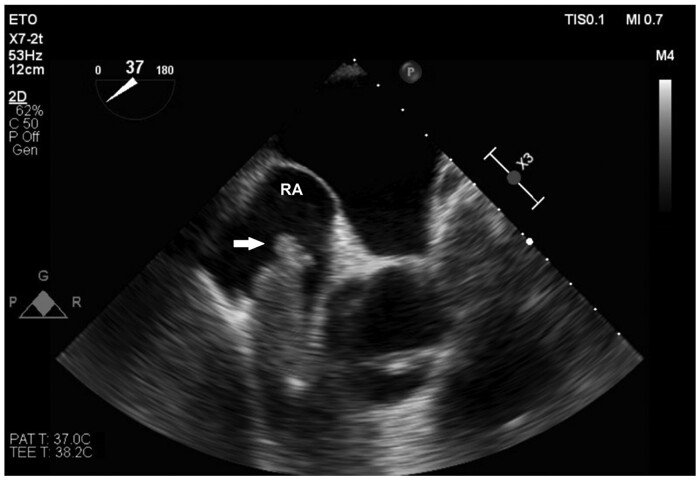
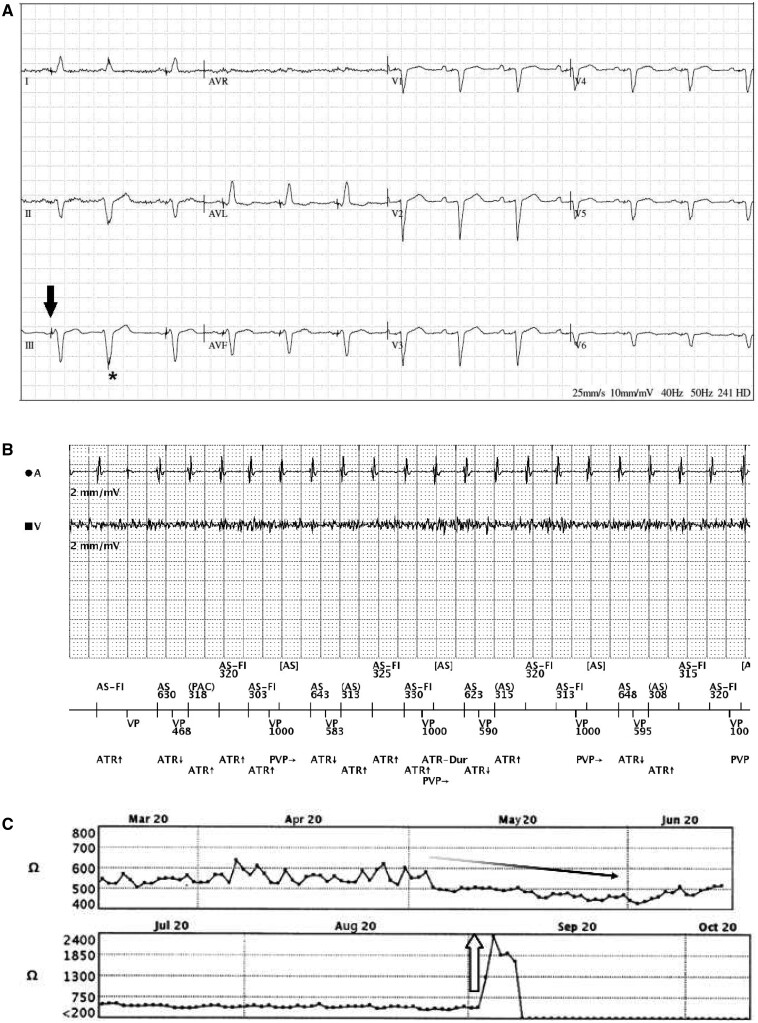
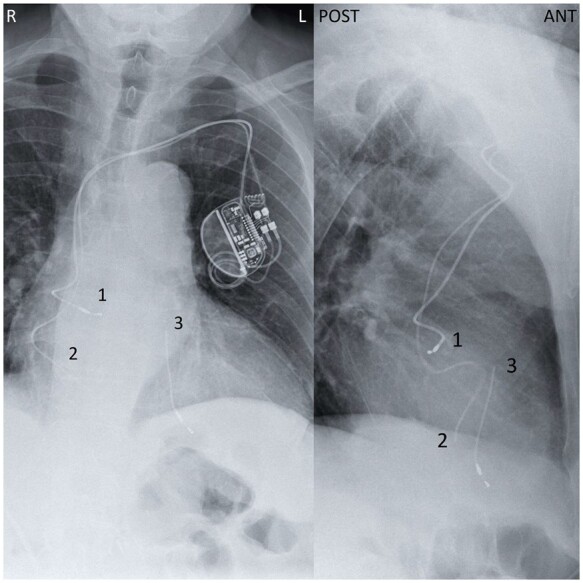
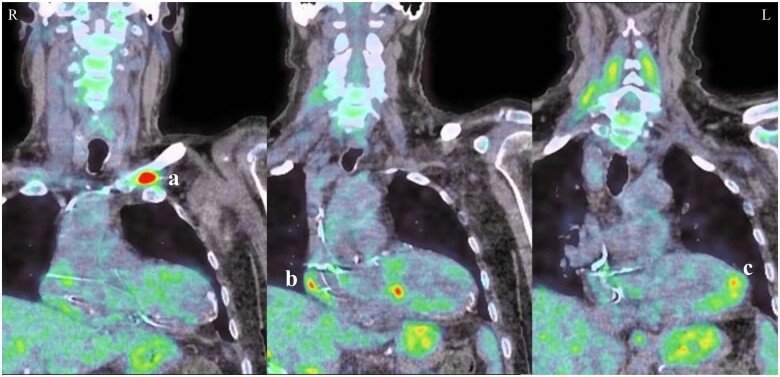
Case summary: We describe the case of a 73-year-old man with a dual-chamber pacemaker presenting with subacute endocarditis and recurrent cholangitis. A few months prior, the patient was diagnosed with localized colon cancer and Streptococcus sanguinis lead endocarditis based on nuclear imaging. He was given prolonged antibiotic therapy and lead explantation was to be performed after sigmoidectomy. During the following weeks, his condition worsened and he was readmitted for biliary sepsis. A chest X-ray revealed, incidentally, a complete ventricular lead rupture. Pacemaker electrogram showed ventricular undersensing, loss of ventricular capture, and high impedance. As his health declined, removal of the pacemaker was deemed unreasonable and the patient died of biliary sepsis in the next few weeks.
Discussion: We describe the case of an asymptomatic intracardiac lead fracture in the setting of colon cancer and a medically managed Streptococcus lead infection. As this complication occurred during lead infection, bacterial damage may have weakened the lead over time. As illustrated by the patient's outcomes, long-term antibiotic therapy should only be used in cases unsuitable for device removal. Complete hardware removal remains the first-line therapy in patients with CIED-related infections.
Keywords: Case report; Fracture; Pacemaker; Pacemaker lead endocarditis; Rupture; Streptococcus sanguinis.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

Similar articles
-
Surgical treatment of pacemaker and defibrillator lead endocarditis: the impact of electrode lead extraction on outcome.Chest. 2003 Oct;124(4):1451-9. doi: 10.1378/chest.124.4.1451. Chest. 2003. PMID: 14555579
-
Managing Complex Pacemaker-Associated Endocarditis With Thromboembolism in Tbilisi, Georgia: A Case Report.Cureus. 2025 Mar 18;17(3):e80804. doi: 10.7759/cureus.80804. eCollection 2025 Mar. Cureus. 2025. PMID: 40255766 Free PMC article.
-
A case of Brucella melitensis endocarditis in a patient with cardiovascular implantable electronic device.Infect Drug Resist. 2018 Mar 9;11:387-390. doi: 10.2147/IDR.S152771. eCollection 2018. Infect Drug Resist. 2018. PMID: 29563819 Free PMC article.
-
Unusual conservative treatment of a complicated pacemaker pocket infection: a case report.J Med Case Rep. 2019 Mar 3;13(1):49. doi: 10.1186/s13256-019-1987-x. J Med Case Rep. 2019. PMID: 30825875 Free PMC article. Review.
-
Candida and cardiovascular implantable electronic devices: a case of lead and native aortic valve endocarditis and literature review.Mycoses. 2015 Nov;58(11):637-41. doi: 10.1111/myc.12391. Epub 2015 Sep 25. Mycoses. 2015. PMID: 26403965 Review.
References
-
- Bongiorni MG, Burri H, Deharo JC, Starck C, Kennergren C, Saghy L. et al.; ESC Scientific Document Group. 2018 EHRA expert consensus statement on lead extraction: recommendations on definitions, endpoints, research trial design, and data collection requirements for clinical scientific studies and registries: endorsed by APHRS/HRS/LAHRS. Europace 2018;20:1217–1217. - PubMed
-
- Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta J-P, Del Zotti F. et al.; ESC Scientific Document Group . 2015 ESC Guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015;36:3075–3128. - PubMed
-
- Sohail MR, Uslan DZ, Khan AH, Friedman PA, Hayes DL, Wilson WR. et al. Management and outcome of permanent pacemaker and implantable cardioverter-defibrillator infections. J Am Coll Cardiol 2007;49:1851–1859. - PubMed
-
- Chamat-Hedemand S, Dahl A, Østergaard L, Arpi M, Fosbøl E, Boel J. et al. Prevalence of infective endocarditis in streptococcal bloodstream infections is dependent on streptococcal species. Circulation 2020;142:720–730. - PubMed
-
- Østergaard L, Bruun NE, Voldstedlund M, Arpi M, Andersen CØ, Schønheyder HC. et al. Prevalence of infective endocarditis in patients with positive blood cultures: a Danish nationwide study. Eur Heart J 2019;40:3237–3244. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials