

Association of Intraindividual Difference in Estimated Glomerular Filtration Rate by Creatinine vs Cystatin C and End-stage Kidney Disease and Mortality
- PMID: 35175342
- PMCID: PMC8855239
- DOI: 10.1001/jamanetworkopen.2021.48940
Association of Intraindividual Difference in Estimated Glomerular Filtration Rate by Creatinine vs Cystatin C and End-stage Kidney Disease and Mortality
Abstract
Importance: As cystatin C is increasingly adopted to estimate glomerular filtration rate (eGFR), clinicians will encounter patients in whom cystatin C-based eGFR (eGFRcys) and creatinine-based eGFR (eGFRcr) differ widely. The clinical implications of these differences, eGFRdiffcys-cr, are unknown.
Objective: To evaluate the associations of eGFRdiffcys-cr with end-stage kidney disease (ESKD) and mortality among individuals with chronic kidney disease (CKD).
Design, setting, and participants: This is a prospective cohort study of 4956 individuals with mild to moderate CKD from 7 clinical centers in the United States who enrolled in the Chronic Renal Insufficiency Cohort (CRIC) Study between 2003 to 2018. Statistical analyses were completed in December 2021.
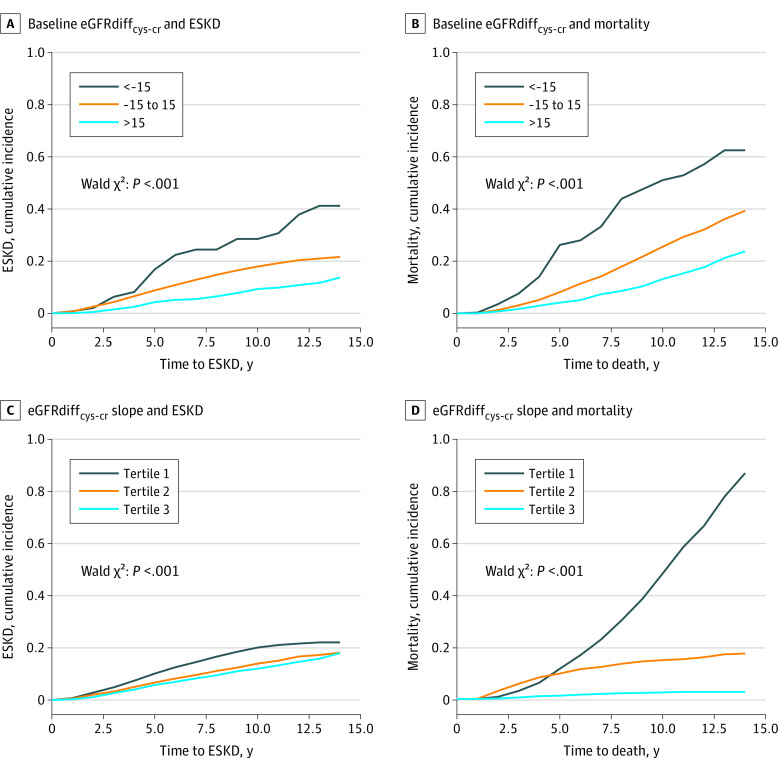
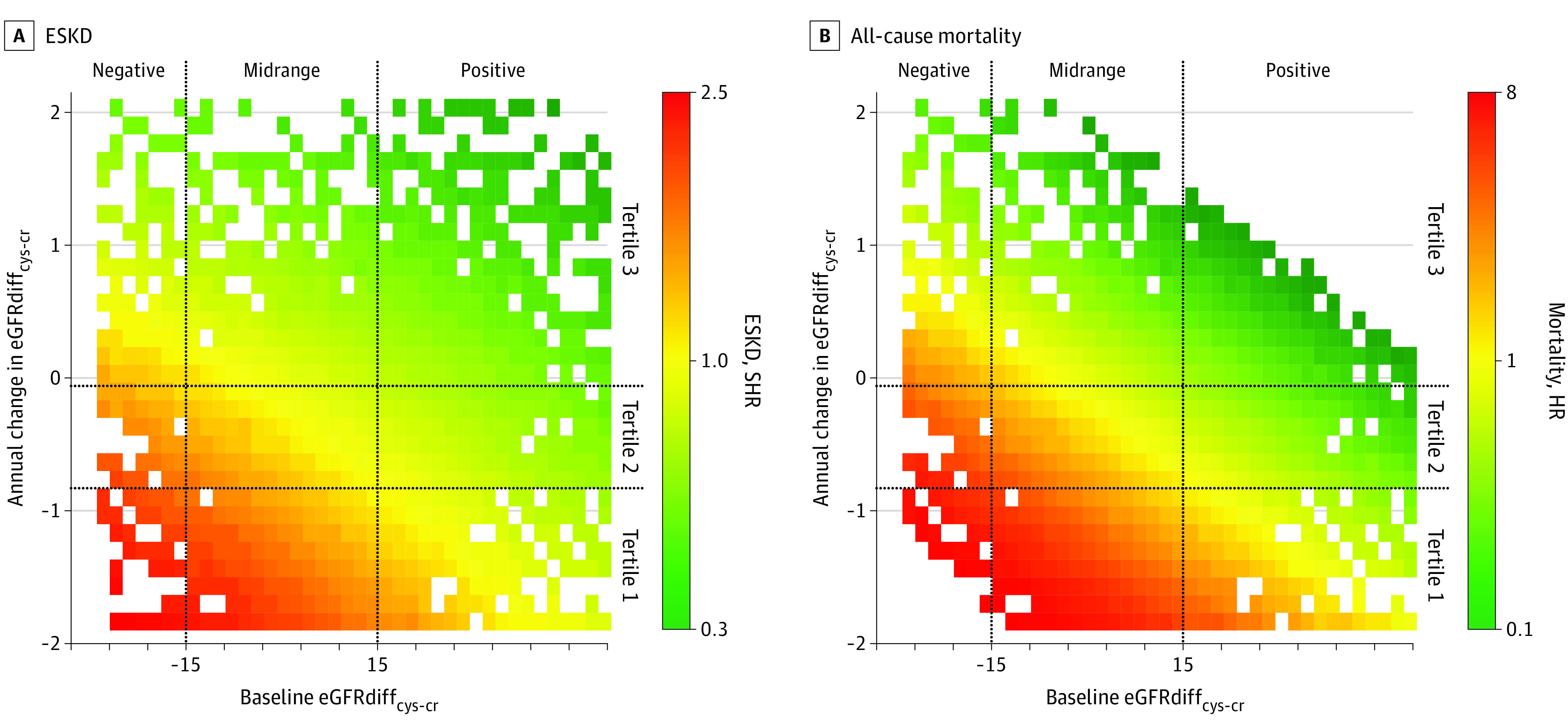
Exposures: eGFRdiffcys-cr (eGFRcys - eGFRcr) was calculated at baseline and annually thereafter for 3 years. Because 15 mL/min/1.73 m2 represents a clinically meaningful difference in eGFR that also distinguishes CKD stages, eGFRdiffcys-cr was categorized as: less than -15 mL/min/1.73 m2, -15 to 15 mL/min/1.73 m2, and 15 mL/min/1.73 m2 or greater.
Main outcomes and measures: The outcomes of ESKD, defined as initiation of maintenance dialysis or receipt of a kidney transplant, and all-cause mortality were adjudicated from study entry until administrative censoring in 2018.
Results: Among 4956 participants with mean (SD) age of 59.5 (10.5) years, 2152 (43.4%) were Black, 515 (10.4%) were Hispanic, and 2113 (42.6%) were White. There were 2156 (43.5%) women and 2800 (56.5%) men. At baseline, eGFRcys and eGFRcr values differed by more than 15 mL/min/1.73 m2 in one-third of participants (1638 participants [33.1%]). Compared with participants with similar baseline eGFRcys and eGFRcr (eGFRdiffcys-cr -15 to 15 mL/min/1.73 m2), those in whom eGFRcys was substantially lower than eGFRcr (eGFRdiffcys-cr < -15 mL/min/1.73 m2) had a higher risk of mortality (hazard ratio [HR], 1.86; 95% CI, 1.40-2.48) while those with eGFRdiffcys-cr of 15 mL/min/1.73 m2 or greater had lower risks of ESKD (subHR [SHR], 0.73; 95% CI, 0.59-0.89) and mortality (HR, 0.68; 95% CI, CI 0.58-0.81). In time-updated analyses, participants with eGFRdiffcys-cr less than -15 mL/min/1.73 m2 had higher risks of ESKD (SHR, 1.83; 95% CI, 1.10-3.04) and mortality (HR, 3.03; 95% CI, 2.19-4.19) compared with participants with similar eGFRcys and eGFRcr. Conversely, participants with eGFRdiffcys-cr of 15 mL/min/1.73 m2 or greater had lower risks of ESKD (SHR, 0.50; 95% CI, 0.35-0.71) and mortality (HR, 0.58; 95% CI, 0.45-0.75). Longitudinal changes in eGFRdiffcys-cr were associated with mortality risk. Compared with participants who had similar slopes by eGFRcys and eGFRcr, those with smaller eGFRcr declines had an 8-fold increased mortality risk (HR, 8.20; 95% CI, 6.37-10.56), and those with larger apparent declines by eGFRcr had a lower mortality risk (HR, 0.14; 95% CI, 0.08-0.24).
Conclusions and relevance: These findings suggest that large differences between eGFRcys and eGFRcr were common in persons with CKD. These differences and their changes over time may be informative of ESKD and mortality risks, warranting monitoring of both eGFRcys and eGFRcr in this high-risk population.
Conflict of interest statement
Figures
References
-
- United States Renal Data System . 2020 Annual Data Report. Accessed January 18, 2022. https://adr.usrds.org/2020
-
- Matsushita K, van der Velde M, Astor BC, et al. ; Chronic Kidney Disease Prognosis Consortium . Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073-2081. doi: 10.1016/S0140-6736(10)60674-5 - DOI - PMC - PubMed
-
- van der Velde M, Matsushita K, Coresh J, et al. ; Chronic Kidney Disease Prognosis Consortium . Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality: a collaborative meta-analysis of high-risk population cohorts. Kidney Int. 2011;79(12):1341-1352. doi: 10.1038/ki.2010.536 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
