

Pregnancy and Reproductive Risk Factors for Cardiovascular Disease in Women
- PMID: 35175837
- PMCID: PMC8870397
- DOI: 10.1161/CIRCRESAHA.121.319895
Pregnancy and Reproductive Risk Factors for Cardiovascular Disease in Women
Abstract
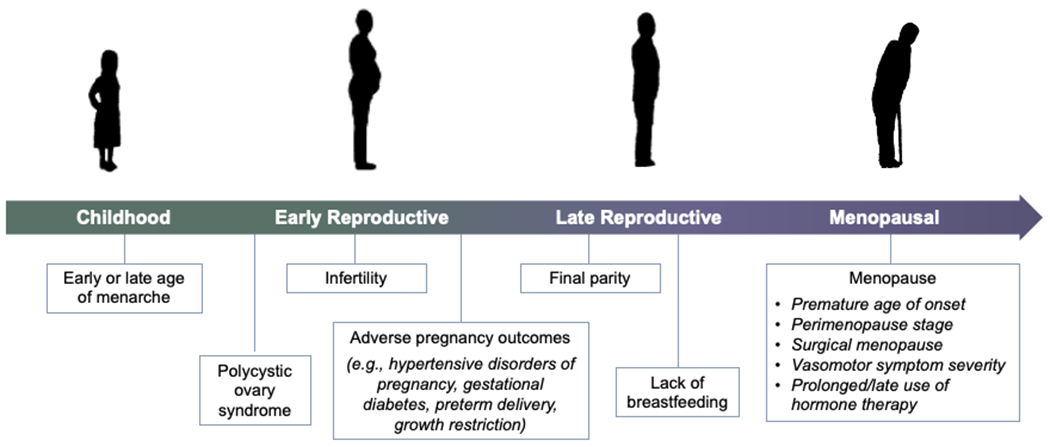
Beyond conventional risk factors for cardiovascular disease, women face an additional burden of sex-specific risk factors. Key stages of a woman's reproductive history may influence or reveal short- and long-term cardiometabolic and cardiovascular trajectories. Early and late menarche, polycystic ovary syndrome, infertility, adverse pregnancy outcomes (eg, hypertensive disorders of pregnancy, gestational diabetes, preterm delivery, and intrauterine growth restriction), and absence of breastfeeding are all associated with increased future cardiovascular disease risk. The menopause transition additionally represents a period of accelerated cardiovascular disease risk, with timing (eg, premature menopause), mechanism, and symptoms of menopause, as well as treatment of menopause symptoms, each contributing to this risk. Differences in conventional cardiovascular disease risk factors appear to explain some, but not all, of the observed associations between reproductive history and later-life cardiovascular disease; further research is needed to elucidate hormonal effects and unique sex-specific disease mechanisms. A history of reproductive risk factors represents an opportunity for comprehensive risk factor screening, refinement of cardiovascular disease risk assessment, and implementation of primordial and primary prevention to optimize long-term cardiometabolic health in women.
Keywords: blood pressure; cardiovascular diseases; pregnancy; risk factors; women.
Figures

References
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Cheng S, Delling FN, et al. Heart disease and stroke statistics-2021 update: A report from the american heart association. Circulation. 2021;143:e254–e743 - PubMed
-
- O’Kelly AC, Honigberg MC. Sex differences in cardiovascular disease and unique pregnancy-associated risk factors in women. Current Treatment Options Cardiovascular Medicine. 2020;22
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Bruan LT, de Ferranti S, Faiella-Tommasino J, Forman DE, et al. 2018 aha/acc/aacvpr/aapa/abc/acpm/ada/ags/apha/aspc/nla/pcna guideline on the management of blood cholesterol: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. Circulation. 2019;139:e1082–e1143 - PMC - PubMed
-
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, Himmelfarb CD, Khera A, Lloyd-Jones D, McEvoy JW, et al. 2019 acc/aha guideline on the primary prevention of cardiovascular disease: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. Circulation. 2019;140:e596–e646 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
