

Assisted Reproductive Technology Surveillance - United States, 2018
- PMID: 35176012
- PMCID: PMC8865855
- DOI: 10.15585/mmwr.ss7104a1
Assisted Reproductive Technology Surveillance - United States, 2018
Abstract
Problem/condition: Since the first U.S. infant conceived with assisted reproductive technology (ART) was born in 1981, both the use of ART and the number of fertility clinics providing ART services have increased steadily in the United States. ART includes fertility treatments in which eggs or embryos are handled in the laboratory (i.e., in vitro fertilization [IVF] and related procedures). Although the majority of infants conceived through ART are singletons, women who undergo ART procedures are more likely than women who conceive naturally to have multiple births because multiple embryos might be transferred. Multiple births can pose substantial risks for both mothers and infants, including obstetric complications, preterm birth (<37 weeks), and low birthweight (<2,500 g). This report provides state-specific information for the United States (including the District of Columbia and Puerto Rico) on ART procedures performed in 2018 and compares birth outcomes that occurred in 2018 (resulting from ART procedures performed in 2017 and 2018) with outcomes for all infants born in the United States in 2018.
Period covered: 2018.
Description of system: In 1995, CDC began collecting data on ART procedures performed in fertility clinics in the United States as mandated by the Fertility Clinic Success Rate and Certification Act of 1992 (Public Law 102-493 [October 24, 1992]). Data are collected through the National ART Surveillance System (NASS), a web-based data collection system developed by CDC. This report includes data from the 50 U.S. states, the District of Columbia, and Puerto Rico.
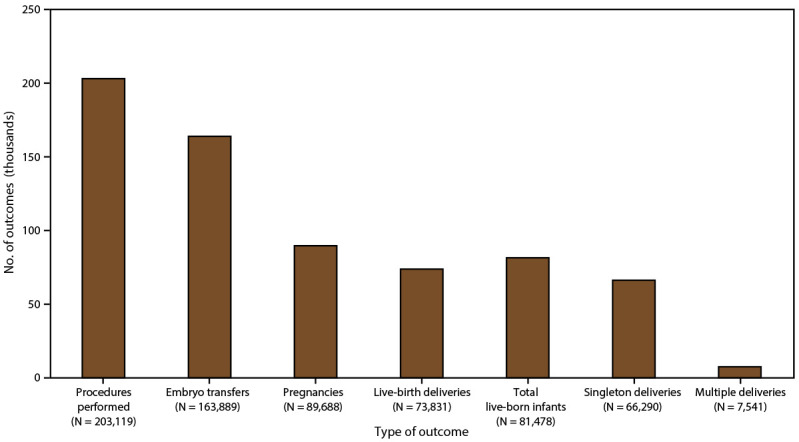
Results: In 2018, a total of 203,119 ART procedures (range: 196 in Alaska to 26,028 in California) were performed in 456 U.S. fertility clinics and reported to CDC. These procedures resulted in 73,831 live-birth deliveries (range: 76 in Puerto Rico and Wyoming to 9,666 in California) and 81,478 infants born (range: 84 in Wyoming to 10,620 in California). Nationally, among women aged 15-44 years, the rate of ART procedures performed was 3,135 per 1 million women. ART use exceeded 1.5 times the national rate in seven states (Connecticut, Illinois, Maryland, Massachusetts, New Jersey, New York, and Rhode Island) and the District of Columbia. ART use rates exceeded the national rate in an additional seven states (California, Delaware, Hawaii, New Hampshire, Utah, Vermont, and Virginia). Nationally, among all ART transfer procedures, the average number of embryos transferred was similar across age groups (1.3 among women aged <35 years, 1.3 among women aged 35-37 years, and 1.4 among women aged >37 years). The national single-embryo transfer (SET) rate among all embryo-transfer procedures was 74.1% among women aged <35 years (range: 28.2% in Puerto Rico to 89.5% in Delaware), 72.8% among women aged 35-37 years (range: 30.6% in Puerto Rico to 93.7% in Delaware), and 66.4% among women aged >37 years (range: 27.1% in Puerto Rico to 85.3% in Delaware). In 2018, ART contributed to 2.0% of all infants born in the United States (range: 0.4% in Puerto Rico to 5.1% in Massachusetts) from procedures performed in 2017 and 2018. Approximately 78.6% of ART-conceived infants were singleton infants. Overall, ART contributed to 12.5% of all multiple births, including 12.5% of all twin births and 13.3% of all triplets and higher-order births. ART-conceived twins accounted for approximately 97.1% (15,532 of 16,001) of all ART-conceived multiple births. The percentage of multiple births was higher among infants conceived with ART (21.4%) than among all infants born in the total birth population (3.3%). Approximately 20.7% (15,532 of 74,926) of ART-conceived infants were twins, and 0.6% (469 of 74,926) were triplets and higher-order multiples. Nationally, infants conceived with ART contributed to 4.2% of all low birthweight (<2,500 g) infants. Among ART-conceived infants, 18.3% were low birthweight compared with 8.3% among all infants. ART-conceived infants contributed to 5.1% of all preterm (gestational age <37 weeks) infants. The percentage of preterm births was higher among infants conceived with ART (26.1%) than among all infants born in the total birth population (10.0%). The percentage of low birthweight among singletons was 8.3% among ART-conceived infants and 6.6% among all infants born. The percentage of preterm births among ART-conceived singleton infants was 14.9% compared with 8.3% among all singleton infants. The percentages of small for gestational age infants was 7.3% among ART-conceived infants compared with 9.4% among all infants.
Interpretation: Although singleton infants accounted for the majority of ART-conceived infants, multiple births from ART varied substantially among states and nationally, contributing to >12% of all twins, triplets, and higher-order multiple infants born in the United States. Because multiple births are associated with higher rates of prematurity than singleton births, the contribution of ART to poor birth outcomes continues to be noteworthy. Although SET rates increased among all age groups, variations in SET rates among states and territories remained, which might reflect variations in embryo-transfer practices among fertility clinics and might in part account for variations in multiple birth rates among states and territories.
Public health action: Reducing the number of embryos transferred and increasing use of SET, when clinically appropriate, can help reduce multiple births and related adverse health consequences for both mothers and infants. Whereas risks to mothers from multiple-birth pregnancy include higher rates of caesarean delivery, gestational hypertension, and gestational diabetes, infants from multiple births are at increased risk for numerous adverse sequelae such as preterm birth, birth defects, and developmental disabilities. Long-term follow-up of ART infants through integration of existing maternal and infant health surveillance systems and registries with data available from NASS might be useful for monitoring adverse outcomes on a population basis.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures

References
-
- CDC. 2018 assisted reproductive technology fertility clinic success rates report. Atlanta, GA: US Department of Health and Human Services, CDC; 2020. https://www.cdc.gov/art/reports/2018/fertility-clinic.html
-
- CDC. 1995 assisted reproductive technology fertility clinic success rates report. Atlanta, GA: US Department of Health and Human Services, CDC; 1997.
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials