

Preclinical Characterization and Phase I Trial Results of a Bispecific Antibody Targeting PD-L1 and 4-1BB (GEN1046) in Patients with Advanced Refractory Solid Tumors
- PMID: 35176764
- PMCID: PMC9662884
- DOI: 10.1158/2159-8290.CD-21-1345
Preclinical Characterization and Phase I Trial Results of a Bispecific Antibody Targeting PD-L1 and 4-1BB (GEN1046) in Patients with Advanced Refractory Solid Tumors
Abstract
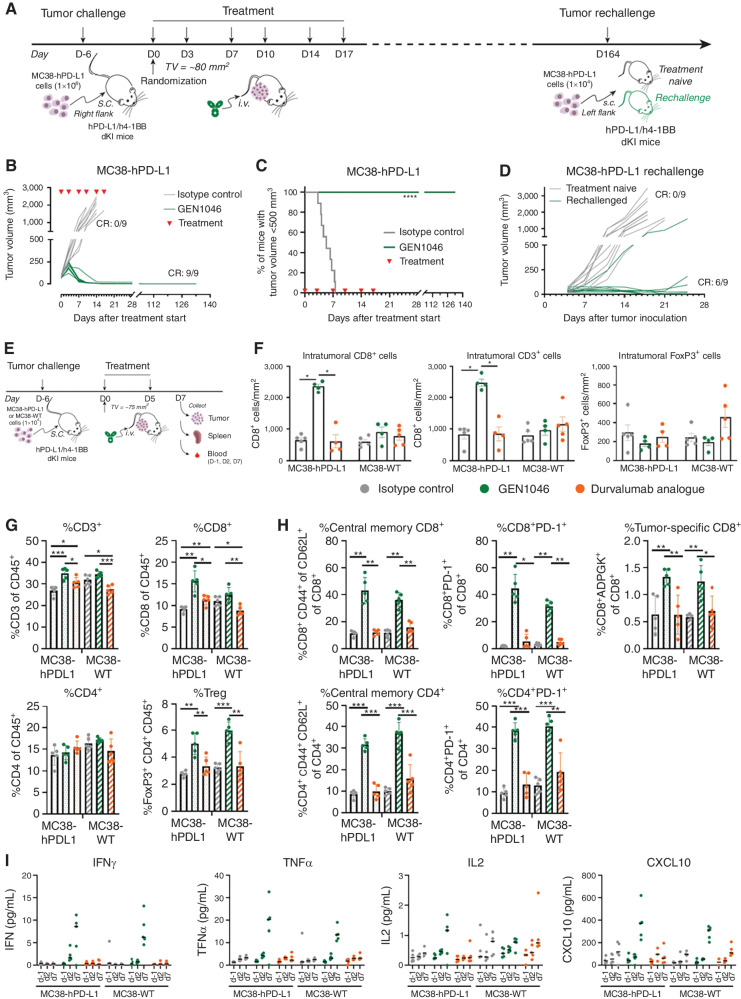
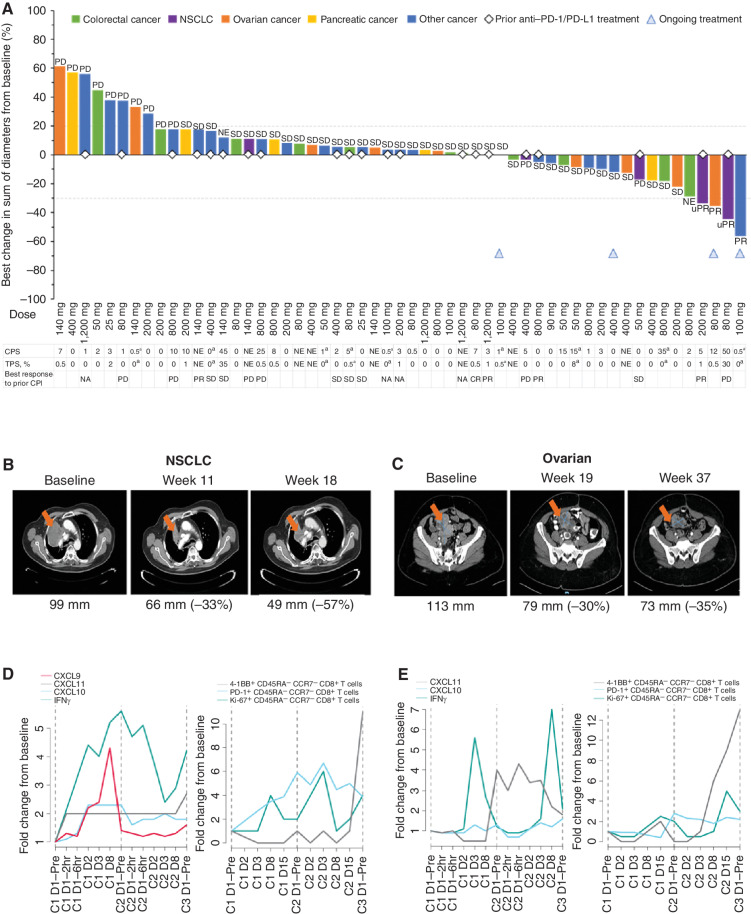
Checkpoint inhibitors (CPI) have revolutionized the treatment paradigm for advanced solid tumors; however, there remains an opportunity to improve response rates and outcomes. In preclinical models, 4-1BB costimulation synergizes with CPIs targeting the programmed cell death protein 1 (PD-1)/programmed cell death ligand 1 (PD-L1) axis by activating cytotoxic T-cell-mediated antitumor immunity. DuoBody-PD-L1×4-1BB (GEN1046) is an investigational, first-in-class bispecific immunotherapy agent designed to act on both pathways by combining simultaneous and complementary PD-L1 blockade and conditional 4-1BB stimulation in one molecule. GEN1046 induced T-cell proliferation, cytokine production, and antigen-specific T-cell-mediated cytotoxicity superior to clinically approved PD-(L)1 antibodies in human T-cell cultures and exerted potent antitumor activity in transplantable mouse tumor models. In dose escalation of the ongoing first-in-human study in heavily pretreated patients with advanced refractory solid tumors (NCT03917381), GEN1046 demonstrated pharmacodynamic immune effects in peripheral blood consistent with its mechanism of action, manageable safety, and early clinical activity [disease control rate: 65.6% (40/61)], including patients resistant to prior PD-(L)1 immunotherapy.
Significance: DuoBody-PD-L1×4-1BB (GEN1046) is a first-in-class bispecific immunotherapy with a manageable safety profile and encouraging preclinical and early clinical activity. With its ability to confer clinical benefit in tumors typically less sensitive to CPIs, GEN1046 may fill a clinical gap in CPI-relapsed or refractory disease or as a combination therapy with CPIs. See related commentary by Li et al., p. 1184. This article is highlighted in the In This Issue feature, p. 1171.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures



Comment in
-
Converting Tumoral PD-L1 into a 4-1BB Agonist for Safer and More Effective Cancer Immunotherapy.Cancer Discov. 2022 May 2;12(5):1184-1186. doi: 10.1158/2159-8290.CD-22-0219. Cancer Discov. 2022. PMID: 35491648
References
-
- Sharma P, Siddiqui BA, Anandhan S, Yadav SS, Subudhi SK, Gao J, et al. The next decade of immune checkpoint therapy. Cancer Discov 2021;11:838–57. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
