

Artificial intelligence stenosis diagnosis in coronary CTA: effect on the performance and consistency of readers with less cardiovascular experience
- PMID: 35177029
- PMCID: PMC8851787
- DOI: 10.1186/s12880-022-00756-y
Artificial intelligence stenosis diagnosis in coronary CTA: effect on the performance and consistency of readers with less cardiovascular experience
Abstract
Background: To investigate the influence of artificial intelligence (AI) based on deep learning on the diagnostic performance and consistency of inexperienced cardiovascular radiologists.
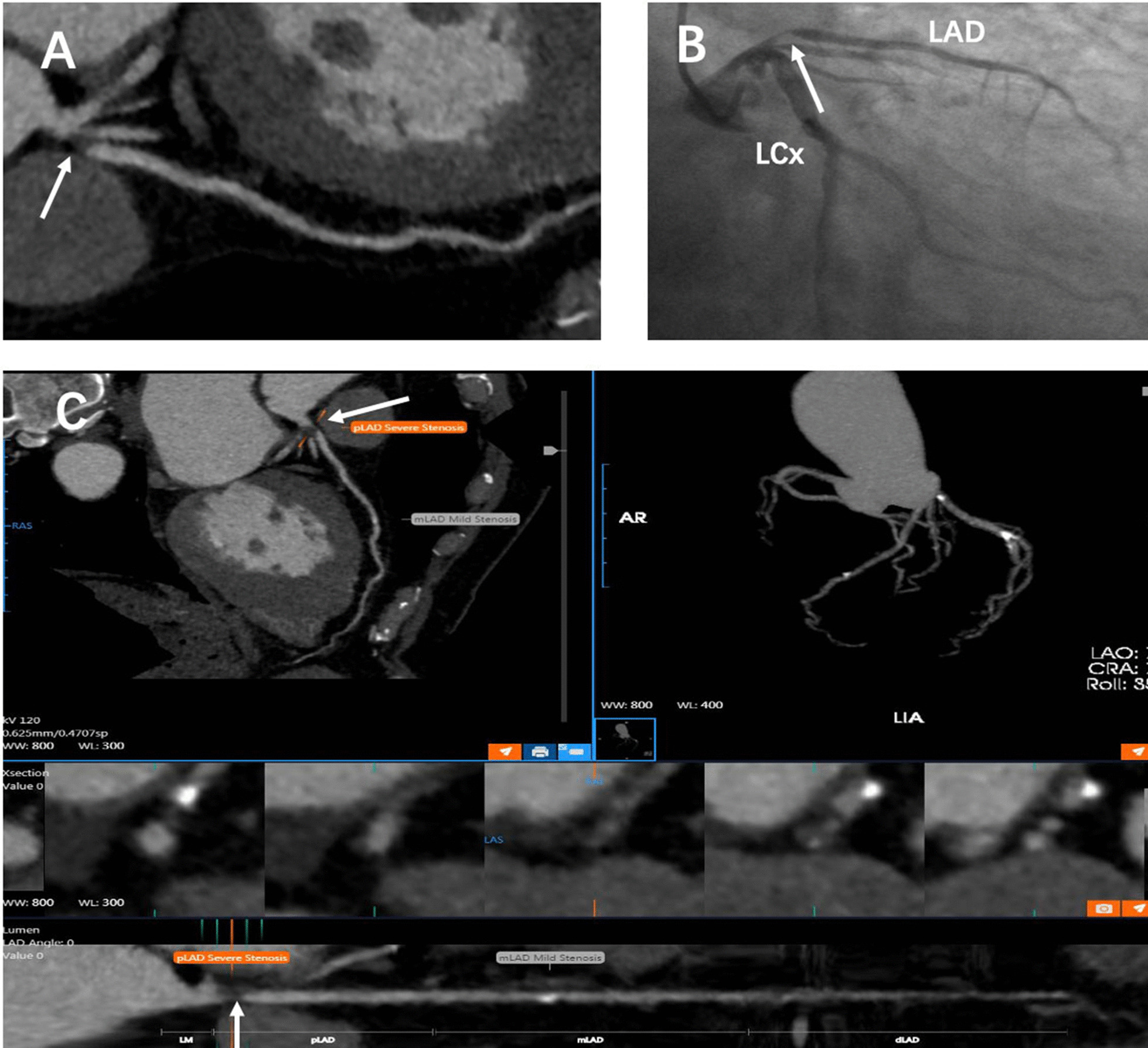
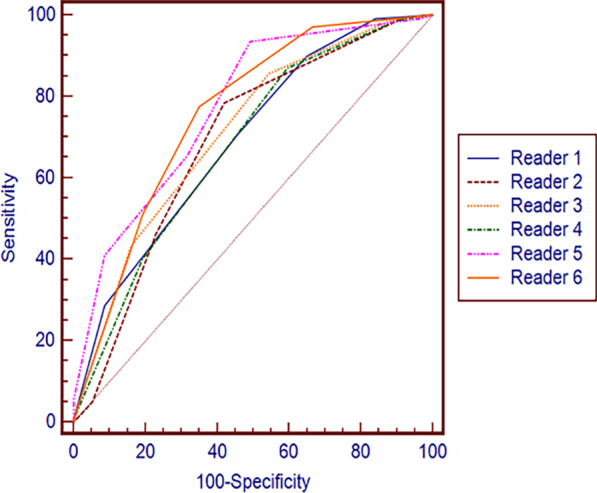
Methods: We enrolled 196 patents who had undergone both coronary computed tomography angiography (CCTA) and invasive coronary angiography (ICA) within 6 months. Four readers with less cardiovascular experience (Reader 1-Reader 4) and two cardiovascular radiologists (level II, Reader 5 and Reader 6) evaluated all images for ≥ 50% coronary artery stenosis, with ICA as the gold standard. Reader 3 and Reader 4 interpreted with AI system assistance, and the other four readers interpreted without the AI system. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy (area under the receiver operating characteristic curve (AUC)) of the six readers were calculated at the patient and vessel levels. Additionally, we evaluated the interobserver consistency between Reader 1 and Reader 2, Reader 3 and Reader 4, and Reader 5 and Reader 6.
Results: The AI system had 94% and 78% sensitivity at the patient and vessel levels, respectively, which were higher than that of Reader 5 and Reader 6. AI-assisted Reader 3 and Reader 4 had higher sensitivity (range + 7.2-+ 16.6% and + 5.9-+ 16.1%, respectively) and NPVs (range + 3.7-+ 13.4% and + 2.7-+ 4.2%, respectively) than Reader 1 and Reader 2 without AI. Good interobserver consistency was found between Reader 3 and Reader 4 in interpreting ≥ 50% stenosis (Kappa value = 0.75 and 0.80 at the patient and vessel levels, respectively). Only Reader 1 and Reader 2 showed poor interobserver consistency (Kappa value = 0.25 and 0.37). Reader 5 and Reader 6 showed moderate agreement (Kappa value = 0.55 and 0.61).
Conclusions: Our study showed that using AI could effectively increase the sensitivity of inexperienced readers and significantly improve the consistency of coronary stenosis diagnosis via CCTA. Trial registration Clinical trial registration number: ChiCTR1900021867. Name of registry: Diagnostic performance of artificial intelligence-assisted coronary computed tomography angiography for the assessment of coronary atherosclerotic stenosis.
Keywords: Artificial intelligence (AI); CCTA; Coronary artery disease; Coronary stenosis; Inexperience readers.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Deep learning powered coronary CT angiography for detecting obstructive coronary artery disease: The effect of reader experience, calcification and image quality.Eur J Radiol. 2021 Sep;142:109835. doi: 10.1016/j.ejrad.2021.109835. Epub 2021 Jun 27. Eur J Radiol. 2021. PMID: 34237493
-
Diagnostic accuracy in coronary CT angiography analysis: artificial intelligence versus human assessment.Open Heart. 2025 Jan 11;12(1):e003115. doi: 10.1136/openhrt-2024-003115. Open Heart. 2025. PMID: 39800437 Free PMC article.
-
The influence of artificial intelligence assistance on the diagnostic performance of CCTA for coronary stenosis for radiologists with different levels of experience.Acta Radiol. 2023 Feb;64(2):496-507. doi: 10.1177/02841851221089263. Epub 2022 Apr 7. Acta Radiol. 2023. PMID: 35389276
-
Accuracy of deep learning in the differential diagnosis of coronary artery stenosis: a systematic review and meta-analysis.BMC Med Imaging. 2024 Sep 16;24(1):243. doi: 10.1186/s12880-024-01403-4. BMC Med Imaging. 2024. PMID: 39285323 Free PMC article.
-
Enhancing Risk Stratification on Coronary Computed Tomography Angiography: The Role of Artificial Intelligence.Clin Ther. 2023 Nov;45(11):1023-1028. doi: 10.1016/j.clinthera.2023.09.019. Epub 2023 Oct 8. Clin Ther. 2023. PMID: 37813776 Review.
Cited by
-
Artificial intelligence in coronary computed tomography angiography: Demands and solutions from a clinical perspective.Front Cardiovasc Med. 2023 Feb 16;10:1120361. doi: 10.3389/fcvm.2023.1120361. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 36873406 Free PMC article. Review.
-
Human AI Teaming for Coronary CT Angiography Assessment: Impact on Imaging Workflow and Diagnostic Accuracy.Diagnostics (Basel). 2023 Nov 30;13(23):3574. doi: 10.3390/diagnostics13233574. Diagnostics (Basel). 2023. PMID: 38066814 Free PMC article.
-
Prospective Human Validation of Artificial Intelligence Interventions in Cardiology: A Scoping Review.JACC Adv. 2024 Aug 28;3(9):101202. doi: 10.1016/j.jacadv.2024.101202. eCollection 2024 Sep. JACC Adv. 2024. PMID: 39372457 Free PMC article.
-
Diagnostic performance of deep learning-based coronary computed tomography angiography in detecting coronary artery stenosis.Int J Cardiovasc Imaging. 2025 May;41(5):979-989. doi: 10.1007/s10554-025-03383-0. Epub 2025 Mar 29. Int J Cardiovasc Imaging. 2025. PMID: 40156689
-
Artificial intelligence-based opportunistic detection of coronary artery stenosis on aortic computed tomography angiography in emergency department patients with acute chest pain.Eur Heart J Open. 2023 Sep 7;3(5):oead088. doi: 10.1093/ehjopen/oead088. eCollection 2023 Sep. Eur Heart J Open. 2023. PMID: 37744954 Free PMC article.
References
-
- de Graaf FR, Schuijf JD, van Velzen JE, Kroft LJ, de Roos A, Reiber JHC, et al. Diagnostic accuracy of 320-row multidetector computed tomography coronary angiography in the non-invasive evaluation of significant coronary artery disease. Eur Heart J. 2010;31(15):1908–1915. doi: 10.1093/eurheartj/ehp571. - DOI - PubMed
-
- Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease. J Am Coll Cardiol. 2008;52(21):1724–1732. doi: 10.1016/j.jacc.2008.07.031. - DOI - PubMed
-
- Hamon M, Biondi-Zoccai GG, Malagutti P, Agostoni P, Morello R, Valgimigli M, et al. Diagnostic performance of multislice spiral computed tomography of coronary arteries as compared with conventional invasive coronary angiography: a meta-analysis. J Am Coll Cardiol. 2006;48(9):1896–1910. doi: 10.1016/j.jacc.2006.08.028. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
