

Postpartum preeclampsia or eclampsia: defining its place and management among the hypertensive disorders of pregnancy
- PMID: 35177218
- PMCID: PMC8857508
- DOI: 10.1016/j.ajog.2020.10.027
Postpartum preeclampsia or eclampsia: defining its place and management among the hypertensive disorders of pregnancy
Abstract
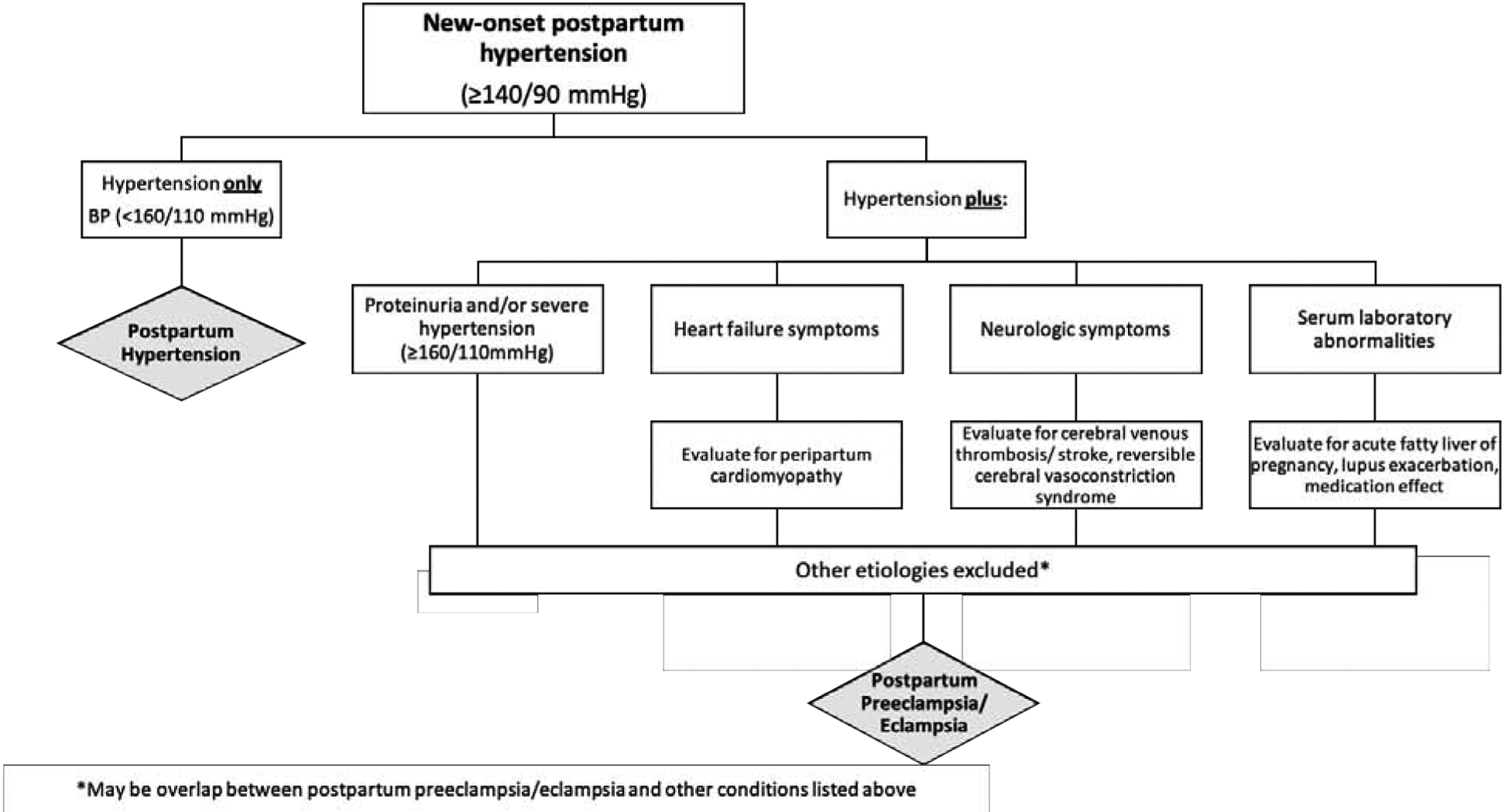
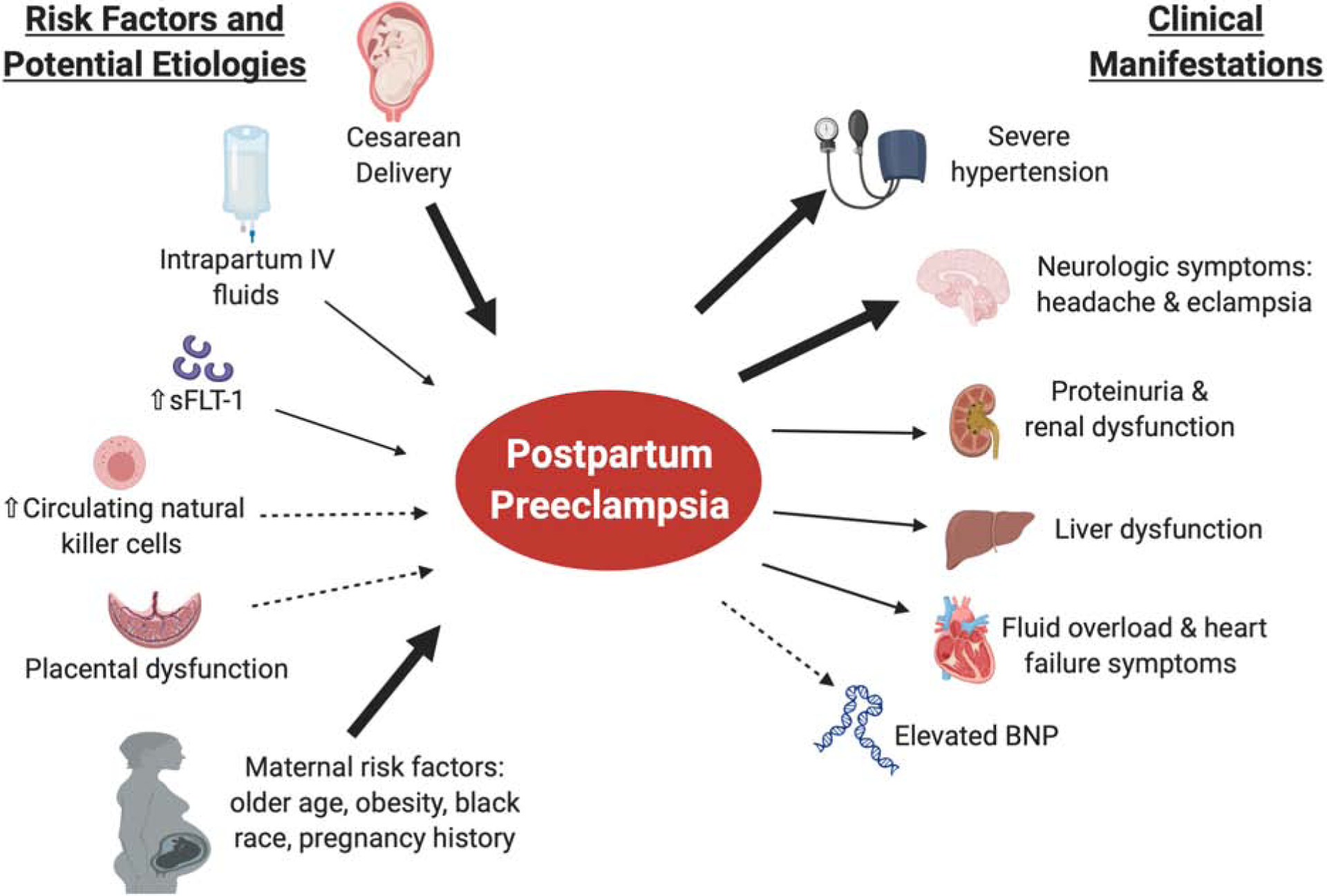
High blood pressure in the postpartum period is most commonly seen in women with antenatal hypertensive disorders, but it can develop de novo in the postpartum time frame. Whether postpartum preeclampsia or eclampsia represents a separate entity from preeclampsia or eclampsia with antepartum onset is unclear. Although definitions vary, the diagnosis of postpartum preeclampsia should be considered in women with new-onset hypertension 48 hours to 6 weeks after delivery. New-onset postpartum preeclampsia is an understudied disease entity with few evidence-based guidelines to guide diagnosis and management. We propose that new-onset hypertension with the presence of any severe features (including severely elevated blood pressure in women with no history of hypertension) be referred to as postpartum preeclampsia after exclusion of other etiologies to facilitate recognition and timely management. Older maternal age, black race, maternal obesity, and cesarean delivery are all associated with a higher risk of postpartum preeclampsia. Most women with delayed-onset postpartum preeclampsia present within the first 7 to 10 days after delivery, most frequently with neurologic symptoms, typically headache. The cornerstones of treatment include the use of antihypertensive agents, magnesium, and diuresis. Postpartum preeclampsia may be associated with a higher risk of maternal morbidity than preeclampsia with antepartum onset, yet it remains an understudied disease process. Future research should focus on the pathophysiology and specific risk factors. A better understanding is imperative for patient care and counseling and anticipatory guidance before hospital discharge and is important for the reduction of maternal morbidity and mortality in the postpartum period.
Keywords: delayed-onset postpartum preeclampsia; hypertension; new-onset postpartum preeclampsia; postpartum; postpartum eclampsia; postpartum hypertension; pregnancy.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Comment in
-
Race as a social construct should not be cited as a risk factor for postpartum preeclampsia.Am J Obstet Gynecol. 2022 Aug;227(2):357-358. doi: 10.1016/j.ajog.2022.03.010. Epub 2022 Mar 10. Am J Obstet Gynecol. 2022. PMID: 35278376 No abstract available.
-
The risk factor is racism, not race.Am J Obstet Gynecol. 2022 Aug;227(2):358-359. doi: 10.1016/j.ajog.2022.03.011. Epub 2022 Mar 10. Am J Obstet Gynecol. 2022. PMID: 35278377 No abstract available.
References
-
- Data on Pregnancy Complications | Pregnancy | Maternal and Infant Health | CDC. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pregnancy-co.... Published 2019. Accessed February 10, 2020.
-
- Hoyert DL, Miniño AM. National Vital Statistics Reports Maternal Mortality in the United States : Changes in Coding, Publication and Data Release, 2018. Natl Vital Stat Reports. 2020;69(2). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
