

Echocardiographic guidance in transcatheter structural cardiac interventions
- PMID: 35177379
- PMCID: PMC9724953
- DOI: 10.4244/EIJ-D-21-00582
Echocardiographic guidance in transcatheter structural cardiac interventions
Abstract
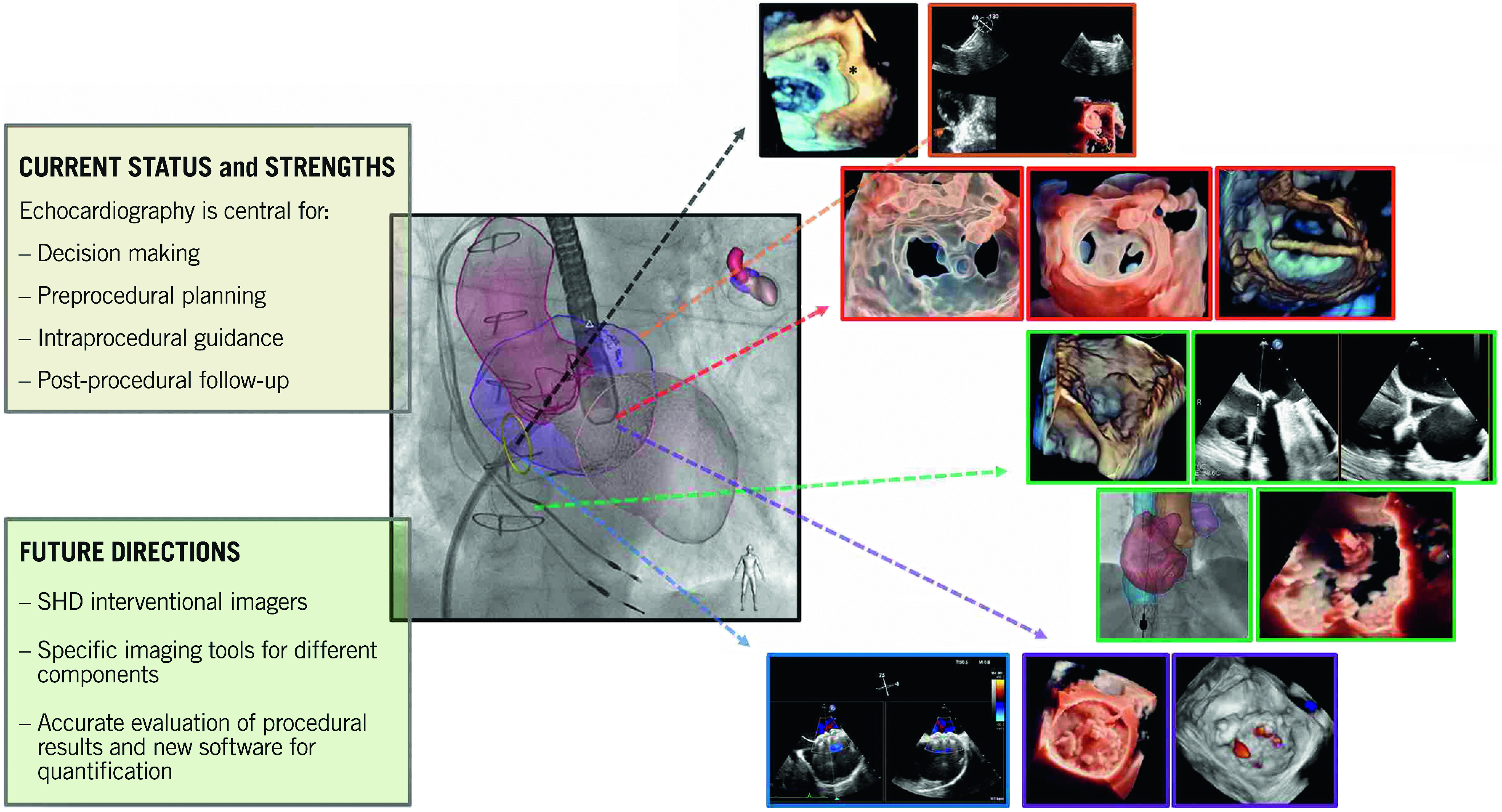
Catheter-based treatment of structural heart diseases (SHD) has seen tremendous advances in the past decades, thanks to the development of new devices and advances in imaging techniques. Today, we have an extensive armamentarium of imaging tools for preprocedural planning, intraprocedural guidance and follow-up of SHD. Intraprocedural guidance is based mainly on transoesophageal echocardiography; however, other imaging modalities are used as complementary or alternative techniques, each of them with its strengths and weaknesses. Thus, a multimodality imaging approach provides added values in this setting. As the field of imaging parallels the continuous technical improvements, this review will describe the state of the art imaging techniques, focusing on echocardiography during procedural guidance of the most common catheter-based interventions, providing tips and tricks for interventional cardiologists: in particular, how to guide transseptal crossing; left atrial appendage closure; transcatheter mitral or tricuspid valve repair or replacement; percutaneous closure of patent foramen ovale and atrial defects; and percutaneous closure of paravalvular leaks. Open challenges for the near future are the need for physicians with specific technical skills and competencies in SHD imaging, more attention to high levels of radiation exposure, and optimisation of intraprocedural and post-procedural evaluation.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures



















References
-
- Rubio-Alvarez V, Limon R, Soni J. Valvulotomias intracardiacas por medio de un cateter [Intracardiac valvulotomy by means of a catheter]. [Article in Undertermined language]. Arch Inst Cardiol Mex. 1953;23:183–92. - PubMed
-
- Vignola PA, Swaye PS, Gosselin AJ. Safe transthoracic left ventricular puncture performed with echocardiographic guidance. Cathet Cardiovasc Diagn. 1980;6:317–24. - PubMed
-
- Hellenbrand WE, Fahey JT, McGowan FX, Weltin GG, Kleinman CS. Transesophageal echocardiographic guidance of transcatheter closure of atrial septal defect. Am J Cardiol. 1990;66:207–13. - PubMed
-
- Ballal RS, Mahan EF, Nanda NC, Dean LS. Utility of transesophageal echocardiography in interatrial septal puncture during percutaneous mitral balloon commissurotomy. Am J Cardiol. 1990;66:230–2. - PubMed
-
- Daoud EG, Kalbfletsch SJ, Hummel JD. Intracardiac echocardiography to guide transseptal left heart catheterization for radiofrequency catheter ablation. J Cardiovasc Electrophysiol. 1999;10:358–63. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous