

A Differential Clinical Benefit Examination of Full Lumbar Endoscopy vs Interspinous Process Spacers in the Treatment of Spinal Stenosis: An Effect Size Meta-Analysis of Clinical Outcomes
- PMID: 35177530
- PMCID: PMC9535687
- DOI: 10.14444/8200
A Differential Clinical Benefit Examination of Full Lumbar Endoscopy vs Interspinous Process Spacers in the Treatment of Spinal Stenosis: An Effect Size Meta-Analysis of Clinical Outcomes
Abstract
Study design: A design-agnostic standardized effect meta-analysis of 48 randomized, prospective, and retrospective studies on clinical outcomes with spinal endoscopic and interspinous process spacer (IPS) surgery.
Objective: The study aimed to provide reference set of Oswestry Disability Index (ODI) and visual analog scale (VAS) effect size data for back and leg pain following endoscopic and IPS decompression for lumbar herniated disc, foraminal, or lateral recess spinal stenosis.
Background: Mechanical low back pain following endoscopic transforaminal decompression may be more reliably reduced by simultaneous posterior column stabilization with IPS.
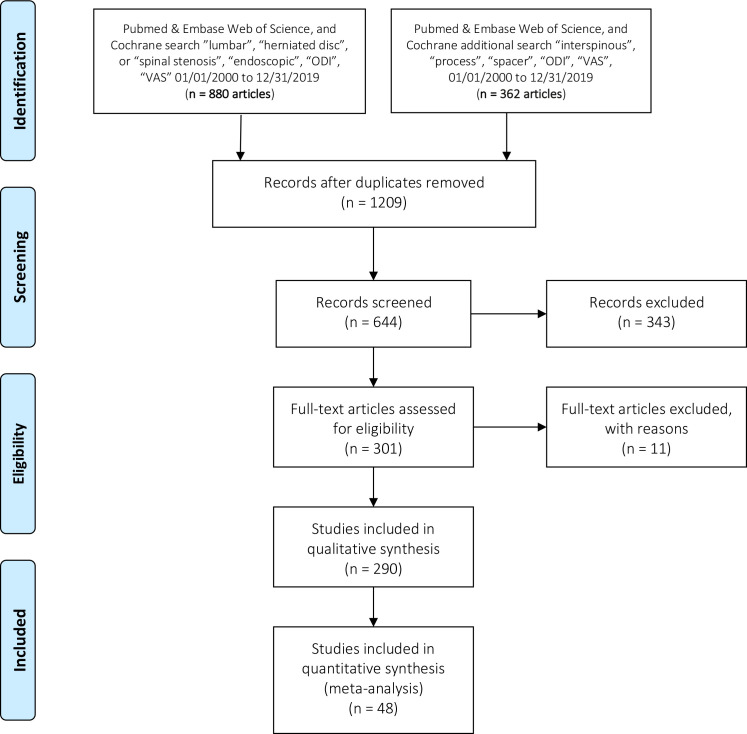
Methods: A systematic search of the PubMed, EMBASE, Web of Science, and the Cochrane Central Register of Controlled Trials from 1 January 2000 to 2 April 2020, identified 880 eligible endoscopy and 362 IPS studies varying in design and metrics. The authors compared calculated standardized effect sizes (Cohen's d) for extracted ODI, VAS-back, and VAS-leg data.
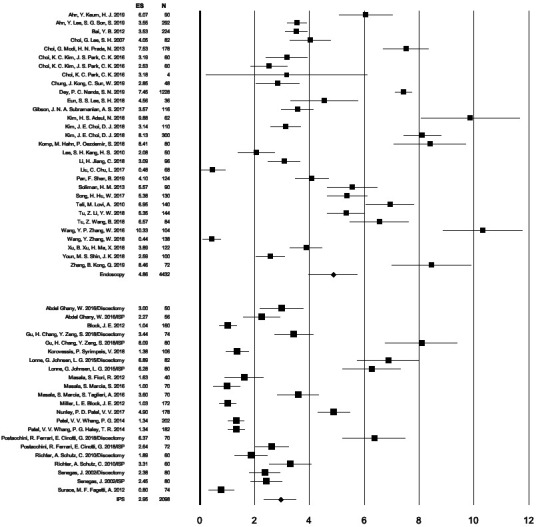
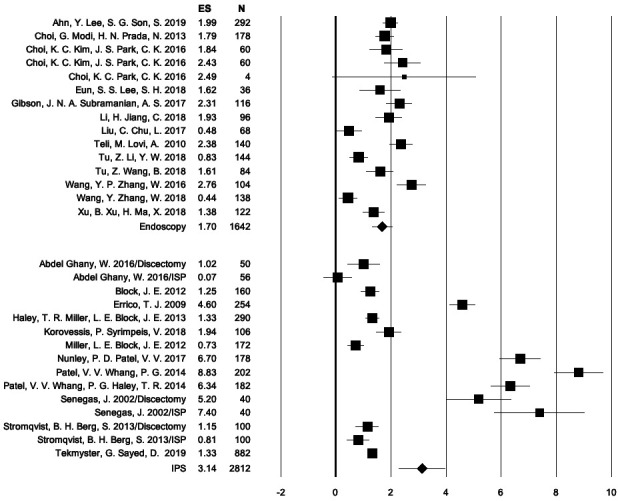
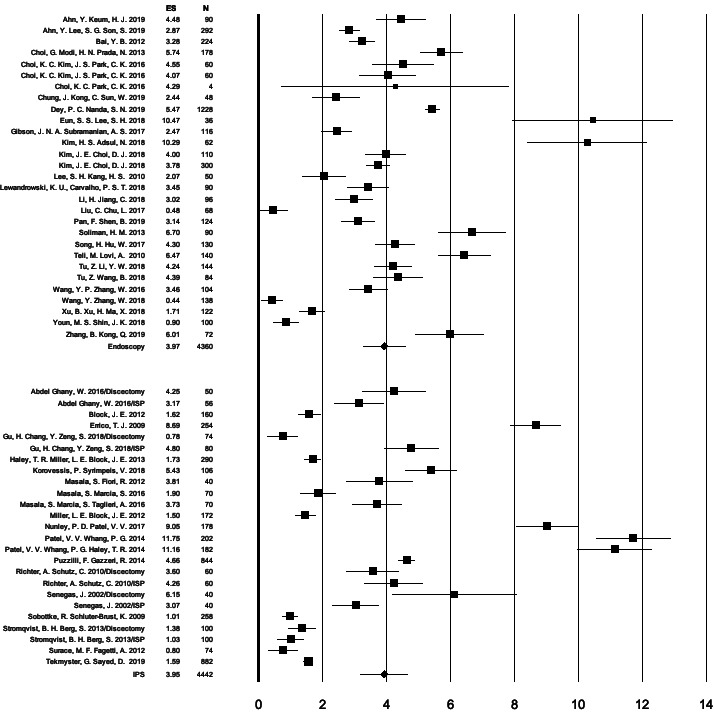
Results: The pooled standardized effect size combining the ODI, VAS-back, and VAS-leg data for the total sample of 19862 data sets from the 30 endoscopy and 18 IPS was 0.877 (95% CI = 0.857-0.898). When stratified by surgery, the combined effect sizes were 0.877 (95% CI = 0.849-0.905) for endoscopic decompression and 0.863 (95% CI = 0.796-0.930; P = 0.056) for IPS implantation. The ODI effect sizes calculated on 6462 samples with directly visualized endoscopic decompression were 0.917 (95% CI = 0.891-0.943) versus 0.798 (95% CI = 0.713-0.883; P < 0.001) with indirect IPS decompression (P < 0.001). The VAS-back effect sizes calculated on 3672 samples were 0.661 (95% CI = 0.585-0.738) for endoscopy and 0.784 (95% CI: 0.644-0.923; P = 0.187) for IPS. The VAS-leg effect sizes calculated on 7890 samples were 0.885 (95% CI = 0.852-0.917) for endoscopic decompression and 0.851 (95% CI = 0.767-0.935; P = 0.427).
Conclusion: Lumbar IPS implantation produces larger reduction in low back pain than spinal endoscopy. On the basis of this meta-analysis, the combination of lumbar transforaminal endoscopy with simultaneous IPS has merits and should be formally investigated in higher grade clinical studies.
Clinical relevance: Meta-analysis on the added clinical benefit of combining lumbar endoscopic decompression with an interspinous process spacer.
Keywords: herniated disc; interspinous process spacer; lumbar endoscopy; meta-analysis; spinal stenosis.
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
Conflict of interest statement
Declaration of Conflicting Interests: The authors report no conflicts of interest related to this work.
Figures
Similar articles
-
Differential Agnostic Effect Size Analysis of Lumbar Stenosis Surgeries.Int J Spine Surg. 2022 Apr;16(2):318-342. doi: 10.14444/8222. Int J Spine Surg. 2022. PMID: 35444041 Free PMC article.
-
Efficacy and Safety of Full-endoscopic Decompression via Interlaminar Approach for Central or Lateral Recess Spinal Stenosis of the Lumbar Spine: A Meta-analysis.Spine (Phila Pa 1976). 2018 Dec 15;43(24):1756-1764. doi: 10.1097/BRS.0000000000002708. Spine (Phila Pa 1976). 2018. PMID: 29794584 Review.
-
Percutaneous transforaminal full endoscopic decompression for the treatment of lumbar spinal stenosis.BMC Musculoskelet Disord. 2020 Aug 14;21(1):546. doi: 10.1186/s12891-020-03566-x. BMC Musculoskelet Disord. 2020. PMID: 32799839 Free PMC article.
-
Transforaminal Endoscopic Discectomy Combined With an Interspinous Process Distraction System for Spinal Stenosis.Int J Spine Surg. 2020 Dec;14(s3):S4-S12. doi: 10.14444/7121. Epub 2020 Oct 29. Int J Spine Surg. 2020. PMID: 33122183 Free PMC article.
-
Full-endoscopic (bi-portal or uni-portal) versus microscopic lumbar decompression laminectomy in patients with spinal stenosis: systematic review and meta-analysis.Eur J Orthop Surg Traumatol. 2020 May;30(4):595-611. doi: 10.1007/s00590-019-02604-2. Epub 2019 Dec 20. Eur J Orthop Surg Traumatol. 2020. PMID: 31863273
References
-
- Dowling Á, Lewandrowski K-U, da Silva FHP, Parra JAA, Portillo DM, Giménez YCP, et al. . Patient selection protocols for endoscopic transforaminal, interlaminar, and translaminar decompression of lumbar spinal stenosis. J Spine Surg. 2020;6(Suppl 1):S120–S132. 10.21037/jss.2019.11.07 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous