

Urine and vaginal microbiota compositions of postmenopausal and premenopausal women differ regardless of recurrent urinary tract infection and renal transplant status
- PMID: 35177690
- PMCID: PMC8854725
- DOI: 10.1038/s41598-022-06646-1
Urine and vaginal microbiota compositions of postmenopausal and premenopausal women differ regardless of recurrent urinary tract infection and renal transplant status
Abstract
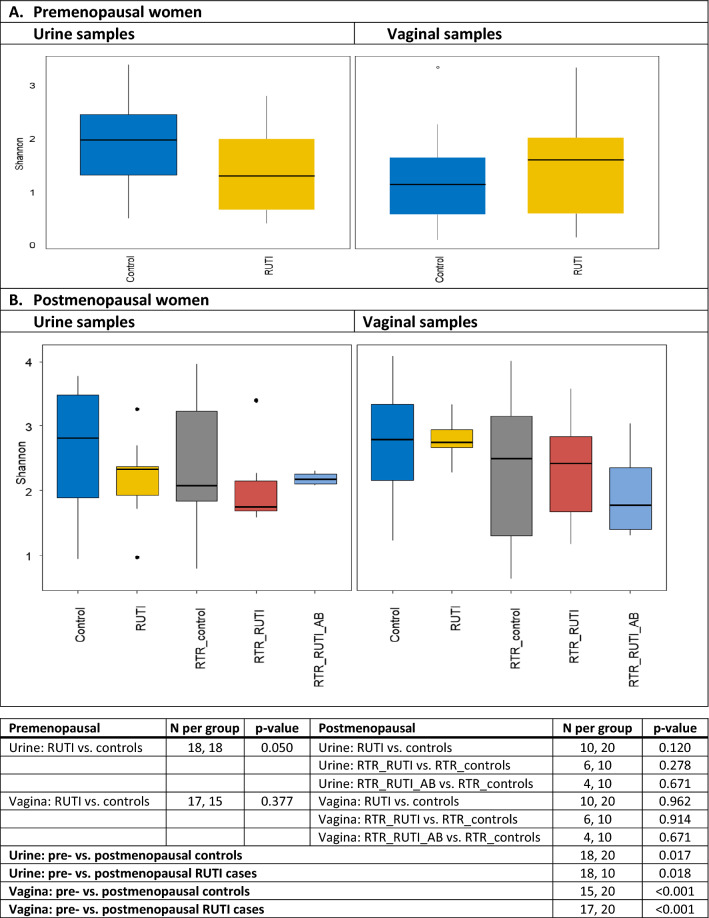
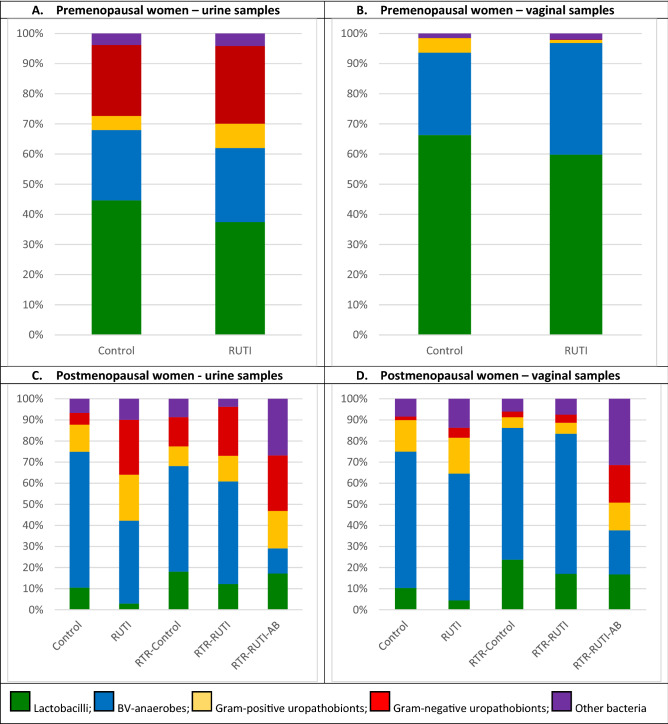
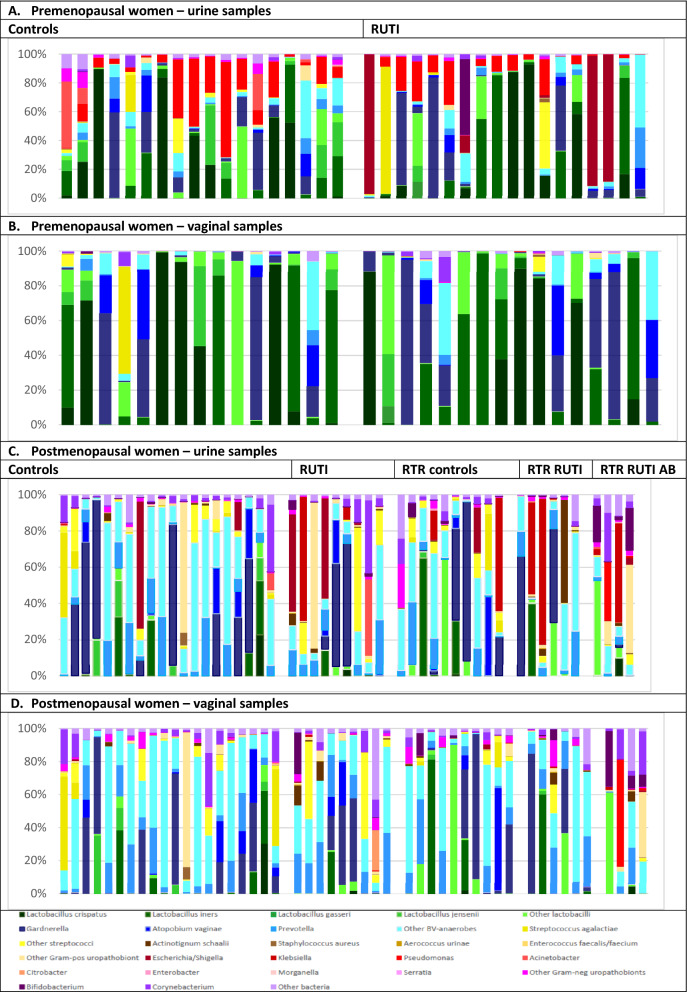
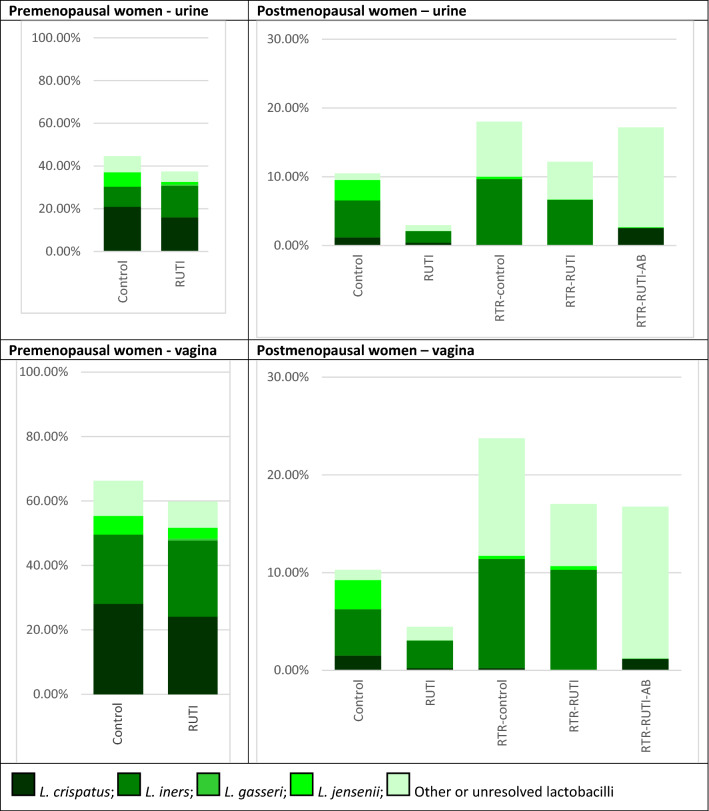
Postmenopausal women and renal transplant recipients are at increased risk of recurrent urinary tract infections (RUTI). Urine and vaginal microbiota of premenopausal controls (N = 18) and RUTI cases (18), and of postmenopausal controls (30) and RUTI cases (20) with and without a renal transplant, were characterized using 16S rRNA sequencing. Participants did not have UTI symptoms at the time of sampling. Gram-negative uropathobionts (predominantly Escherichia/Shigella, Pseudomonas, Klebsiella, and Acinetobacter) had a much higher mean relative abundance in urine than vaginal samples, especially in premenopausal women. No statistically significant differences in mean relative abundances of bacterial groups were found within the premenopausal group or within the postmenopausal group by RUTI or renal transplant status without chronic antibiotic use. Comparing postmenopausal to premenopausal women, mean relative abundances of lactobacilli (especially L. crispatus) in urine and vaginal samples and of Gram-negative uropathobionts in urine were lower, and of BV-anaerobes and Gram-positive uropathobionts in urine and vaginal samples were higher. While RUTI in premenopausal women is predominantly caused by Escherichia, the causative organisms in postmenopausal women are likely more diverse. The relative importance of individual organisms is currently unknown. We recommend that future studies, including intervention studies, include longitudinal microbiota assessments.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
