

Immunopathological signatures in multisystem inflammatory syndrome in children and pediatric COVID-19
- PMID: 35177862
- PMCID: PMC9119950
- DOI: 10.1038/s41591-022-01724-3
Immunopathological signatures in multisystem inflammatory syndrome in children and pediatric COVID-19
Abstract
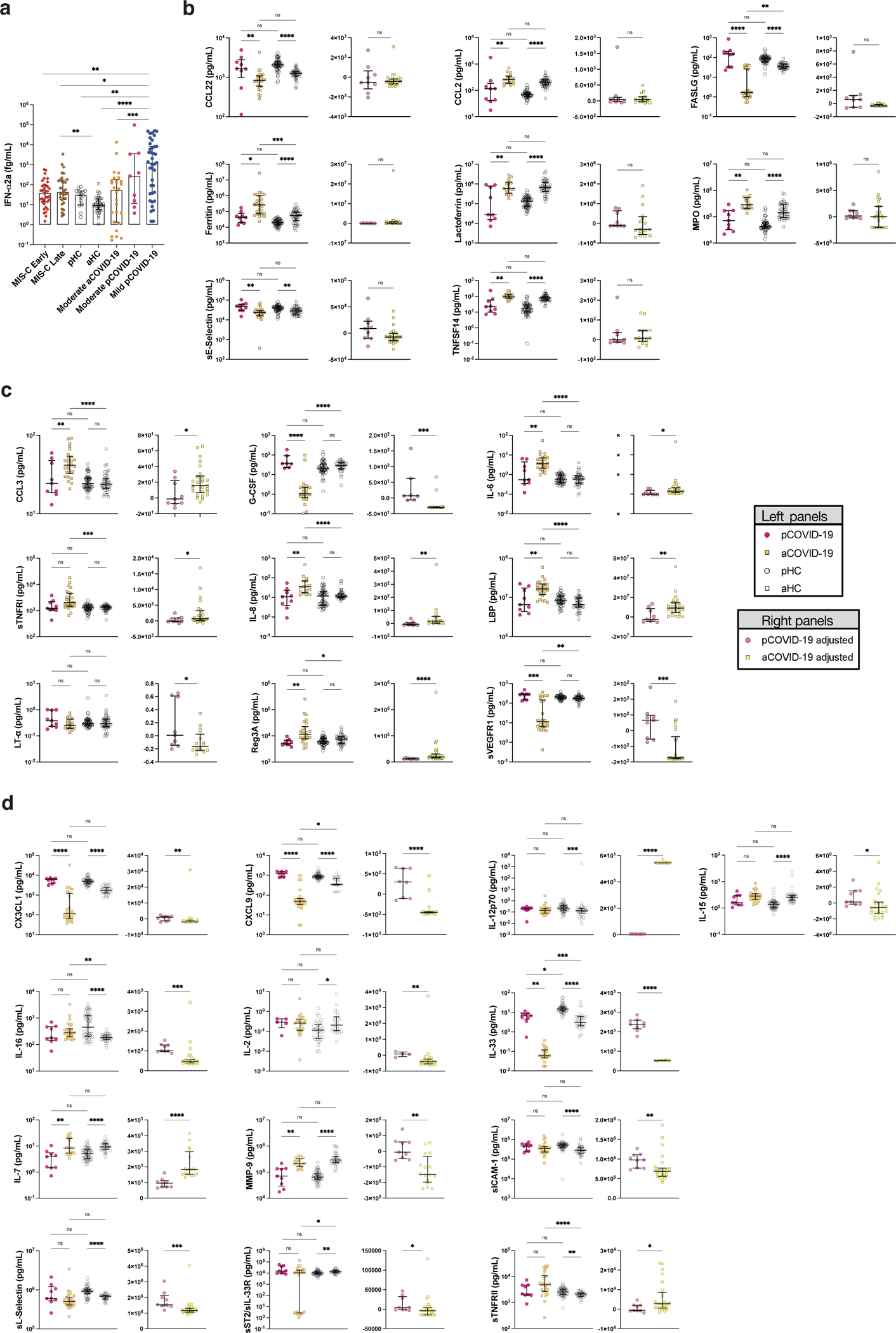
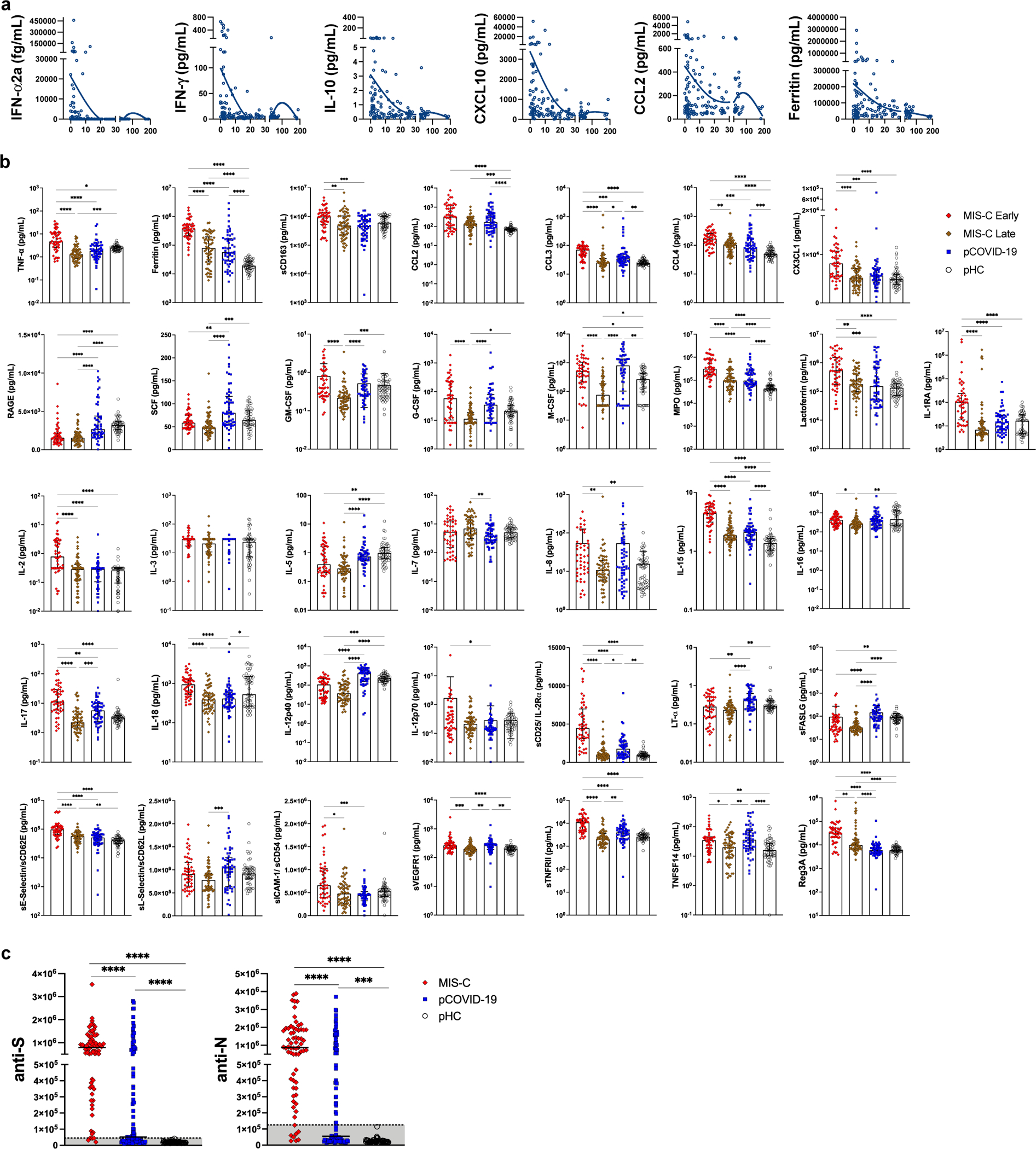
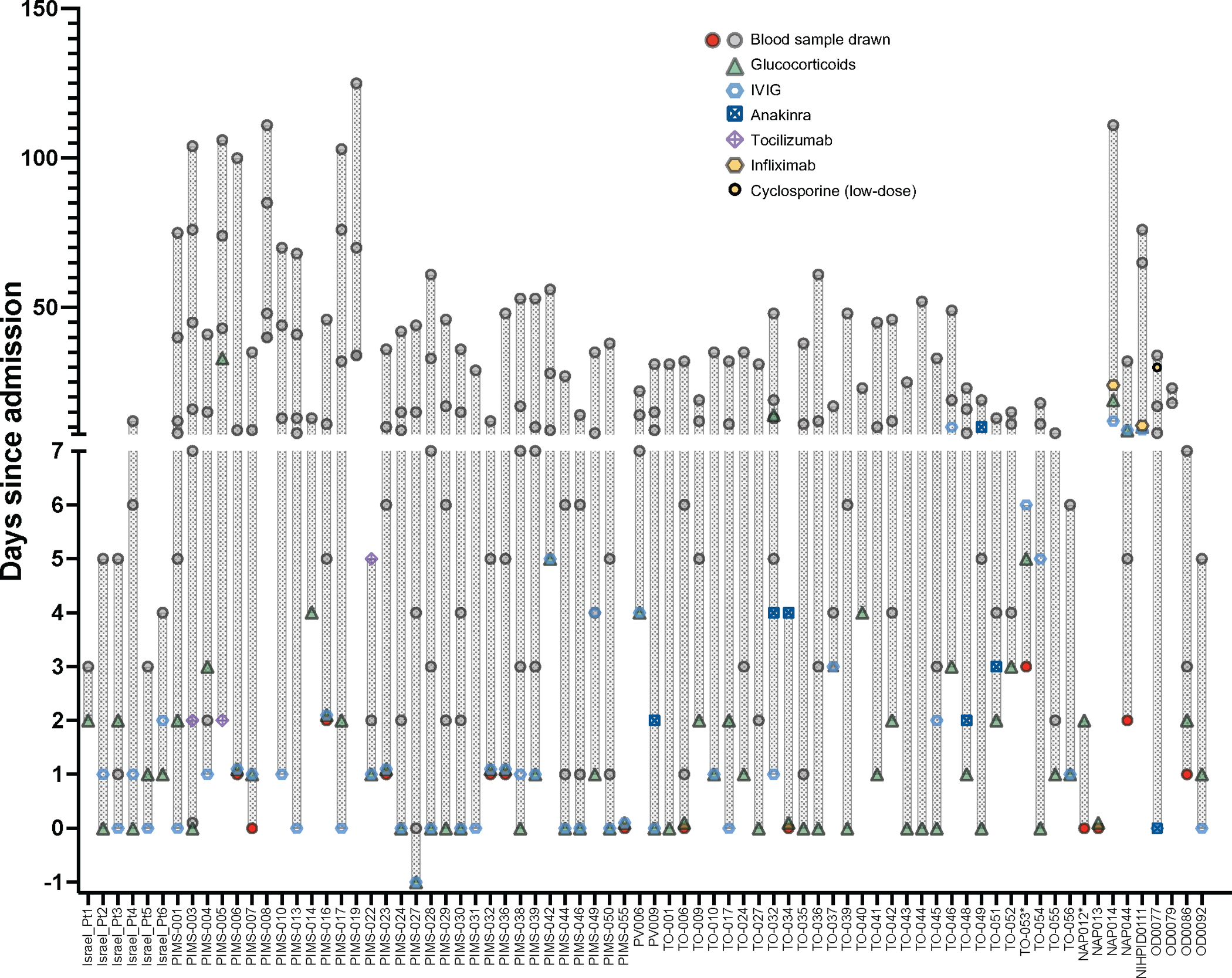
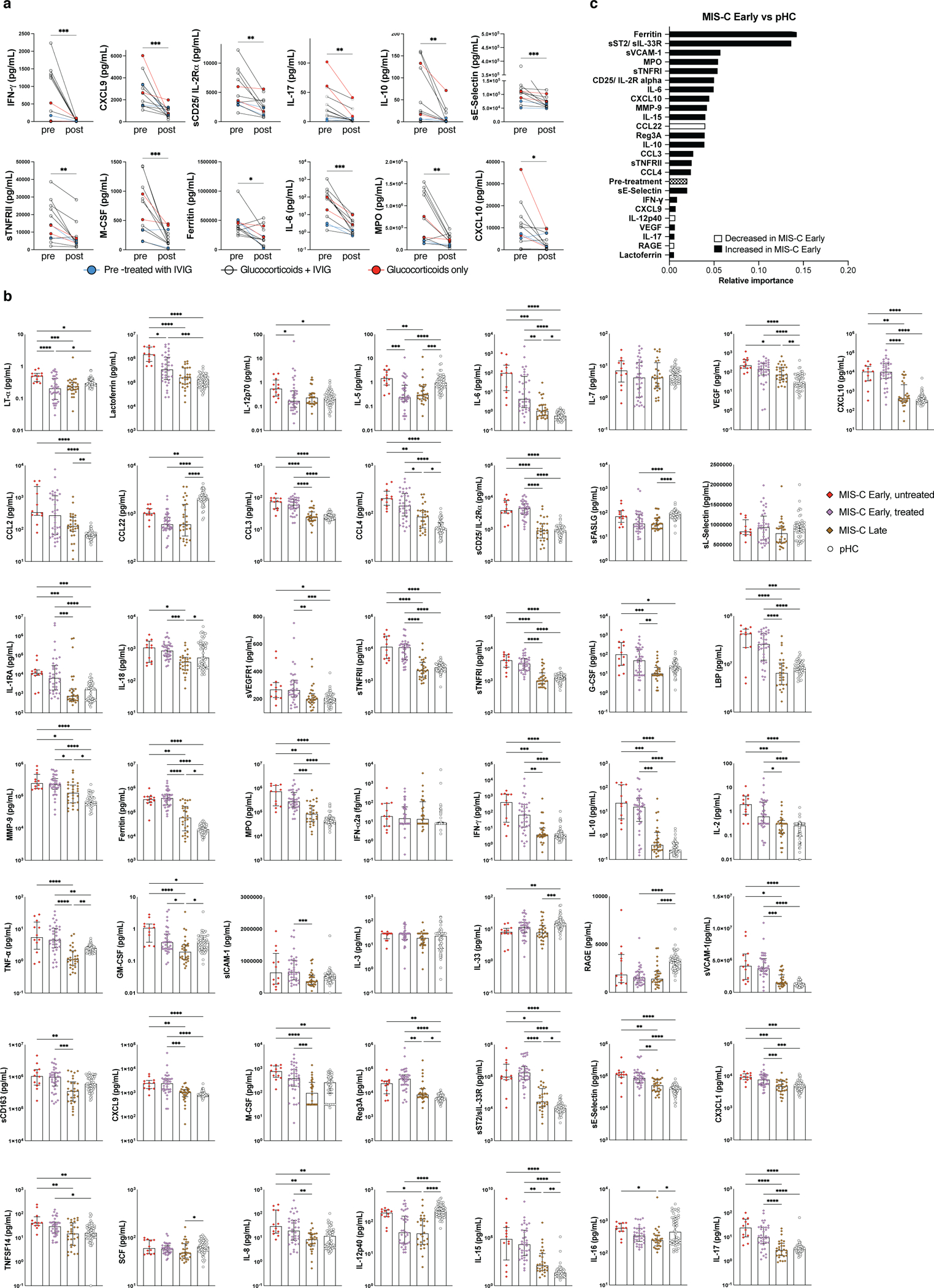
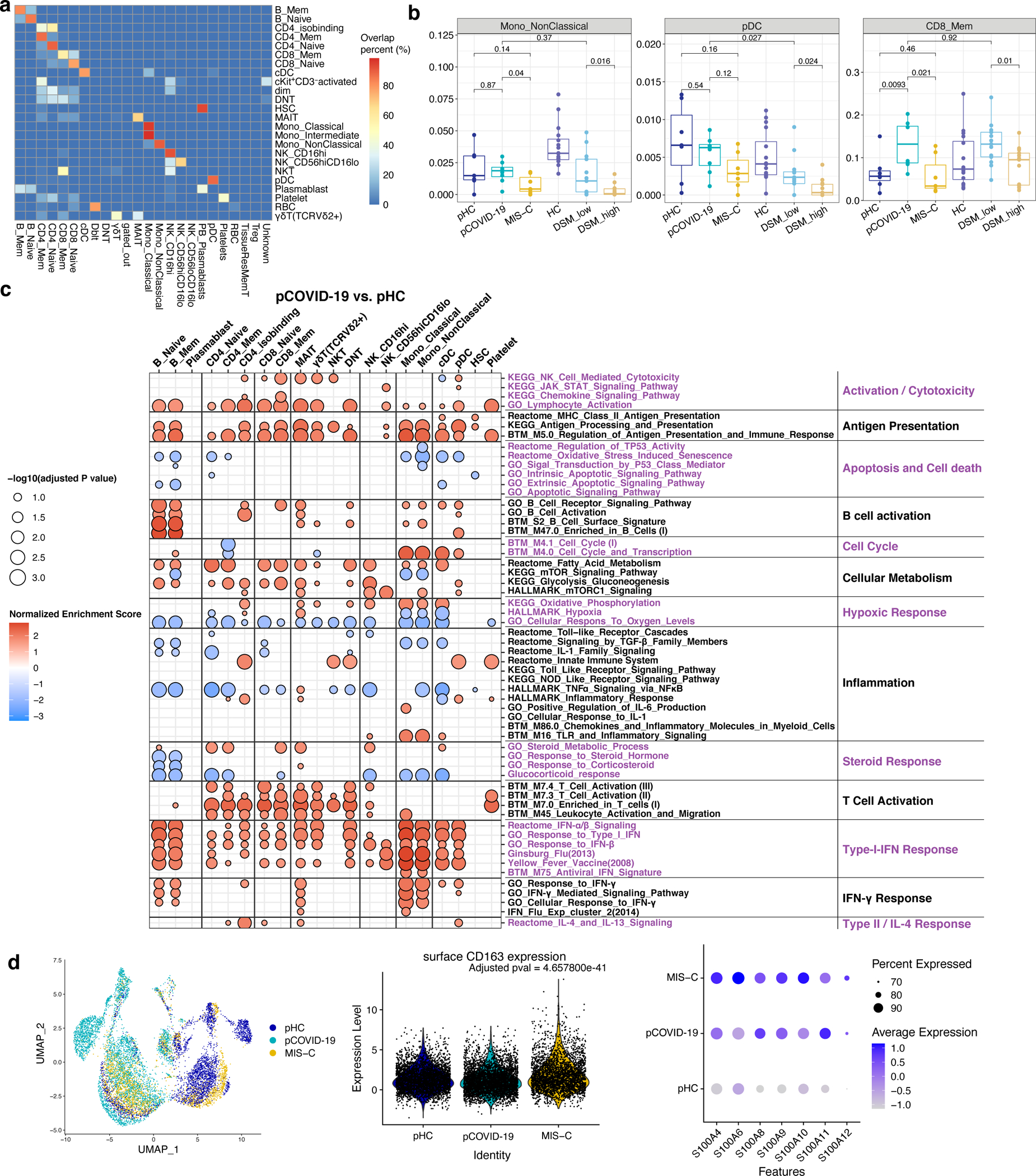
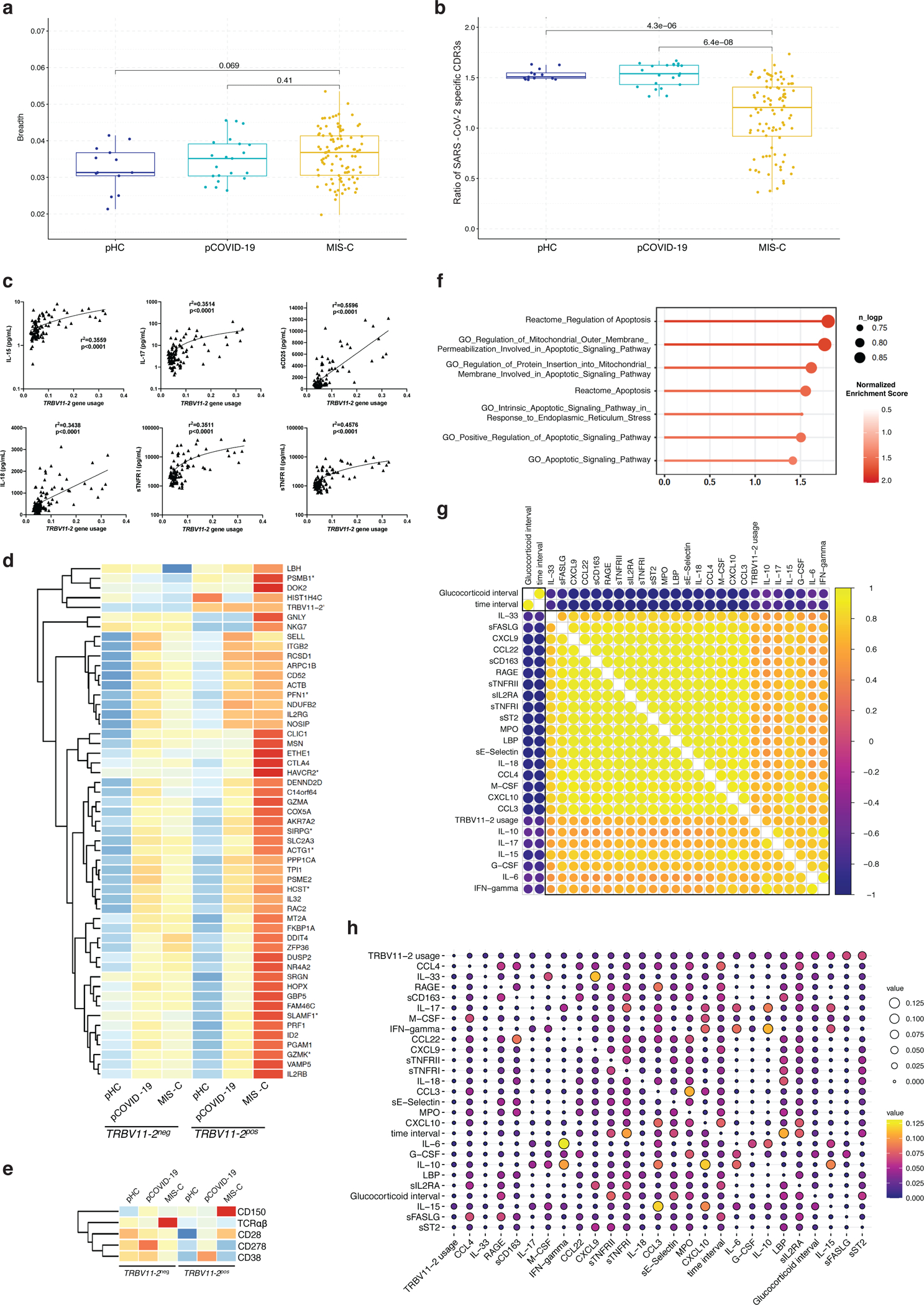
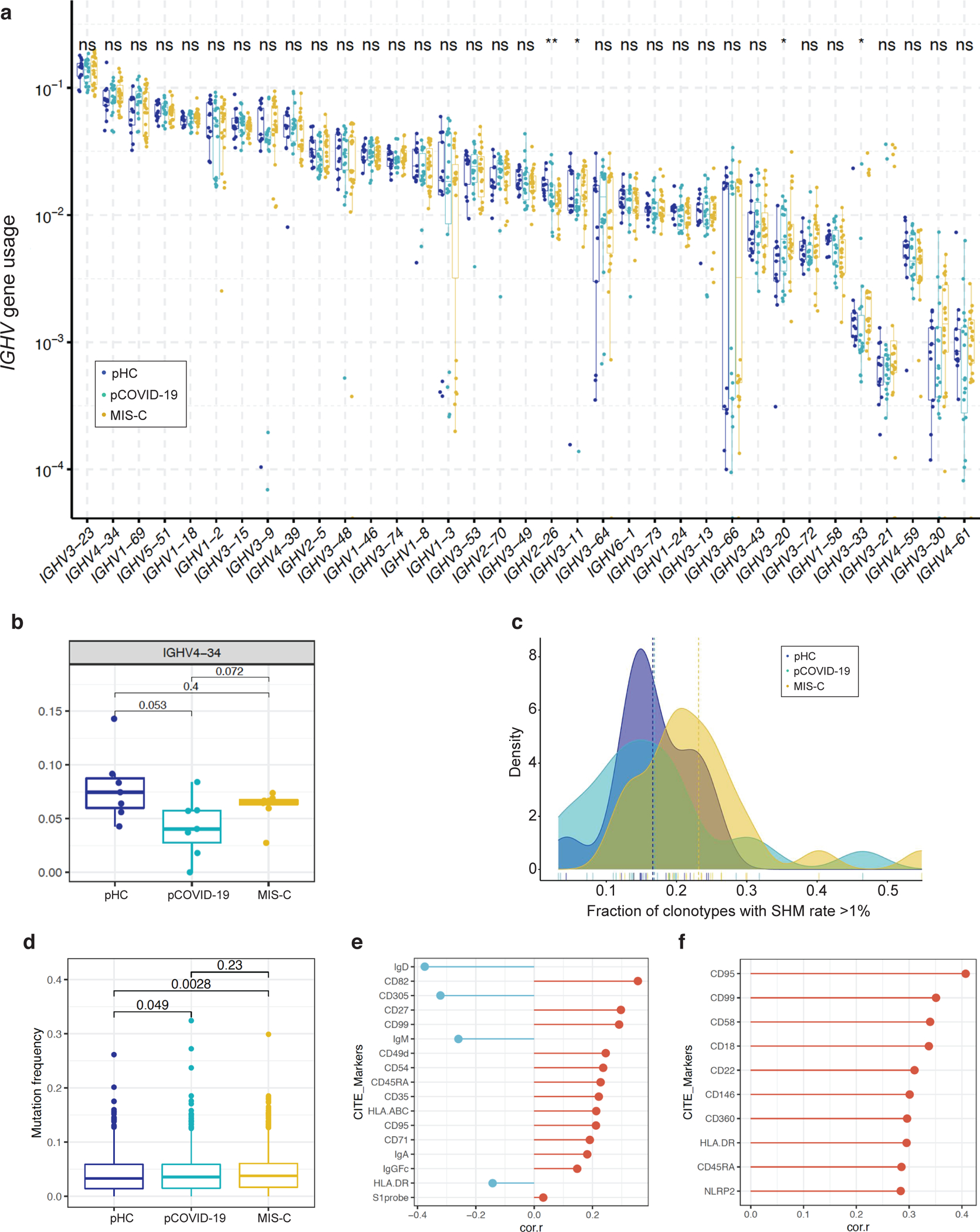
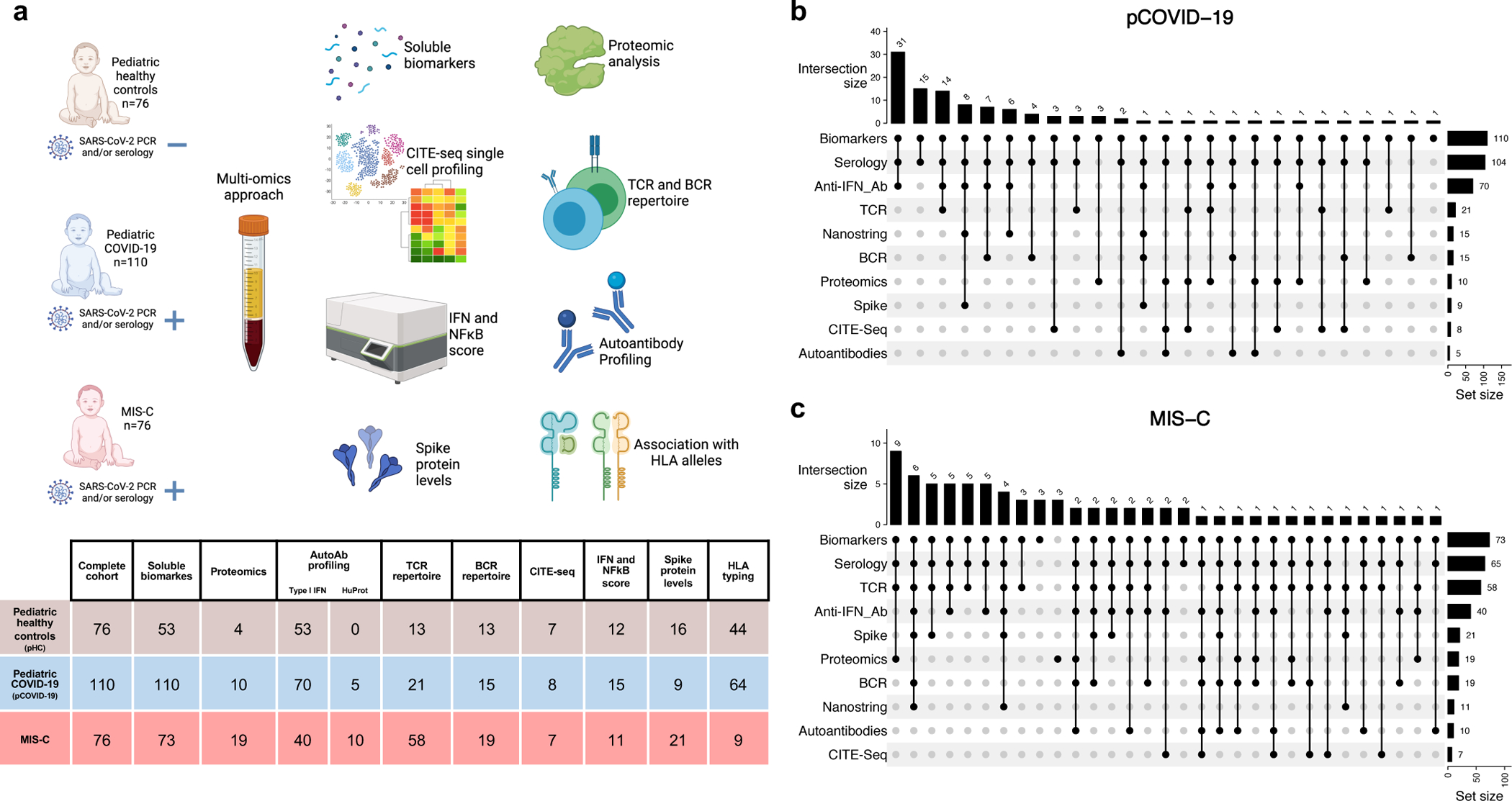
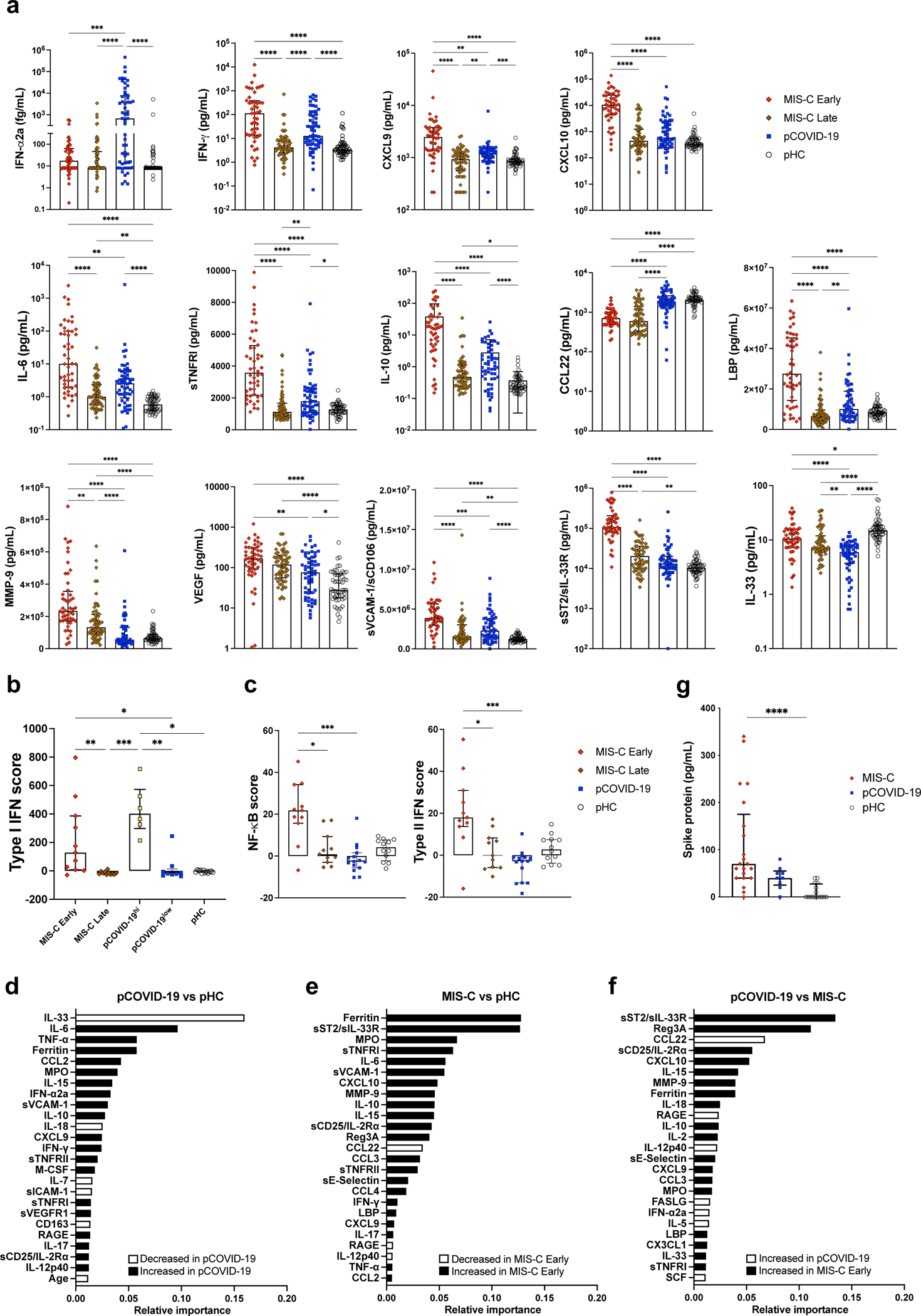
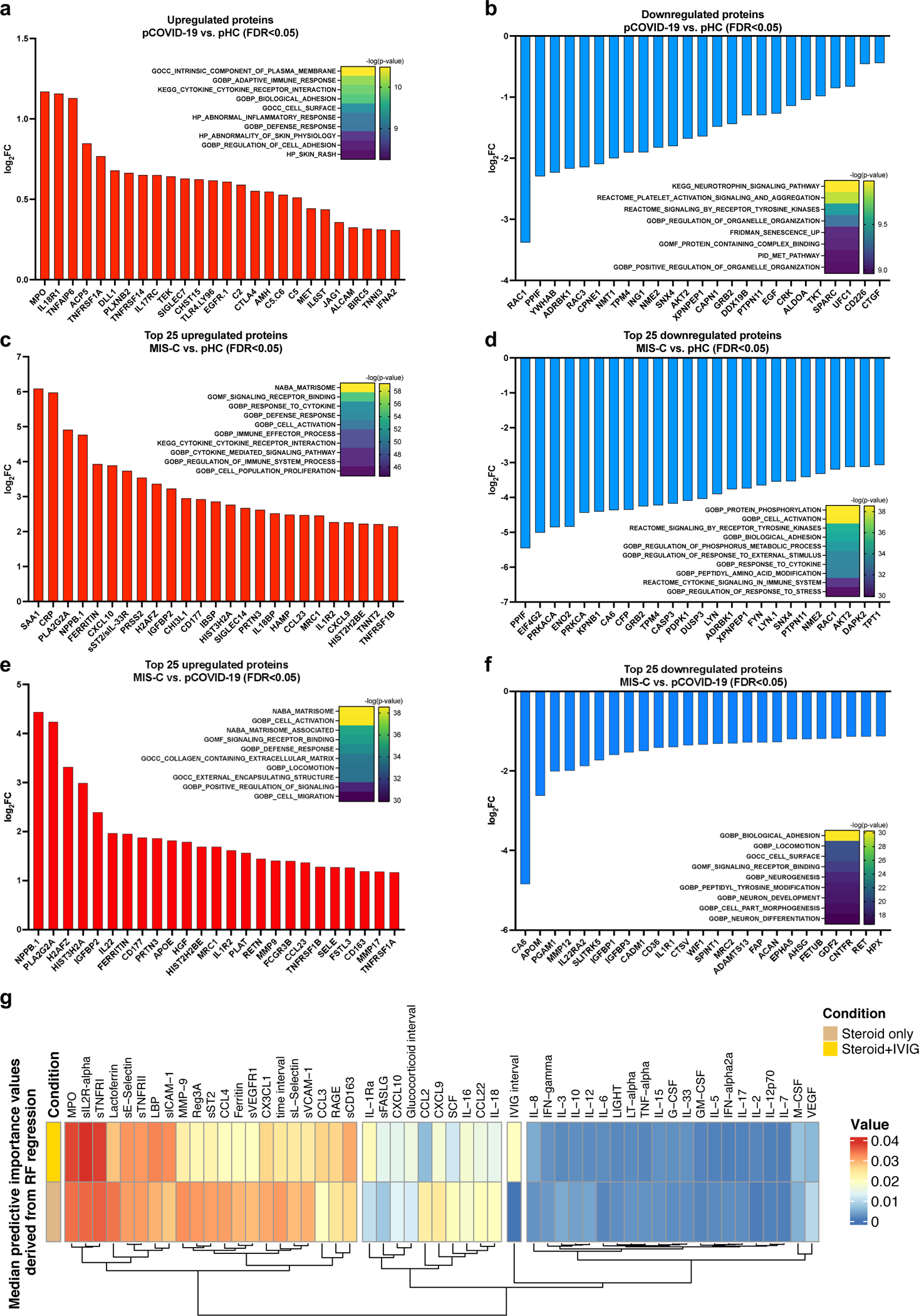
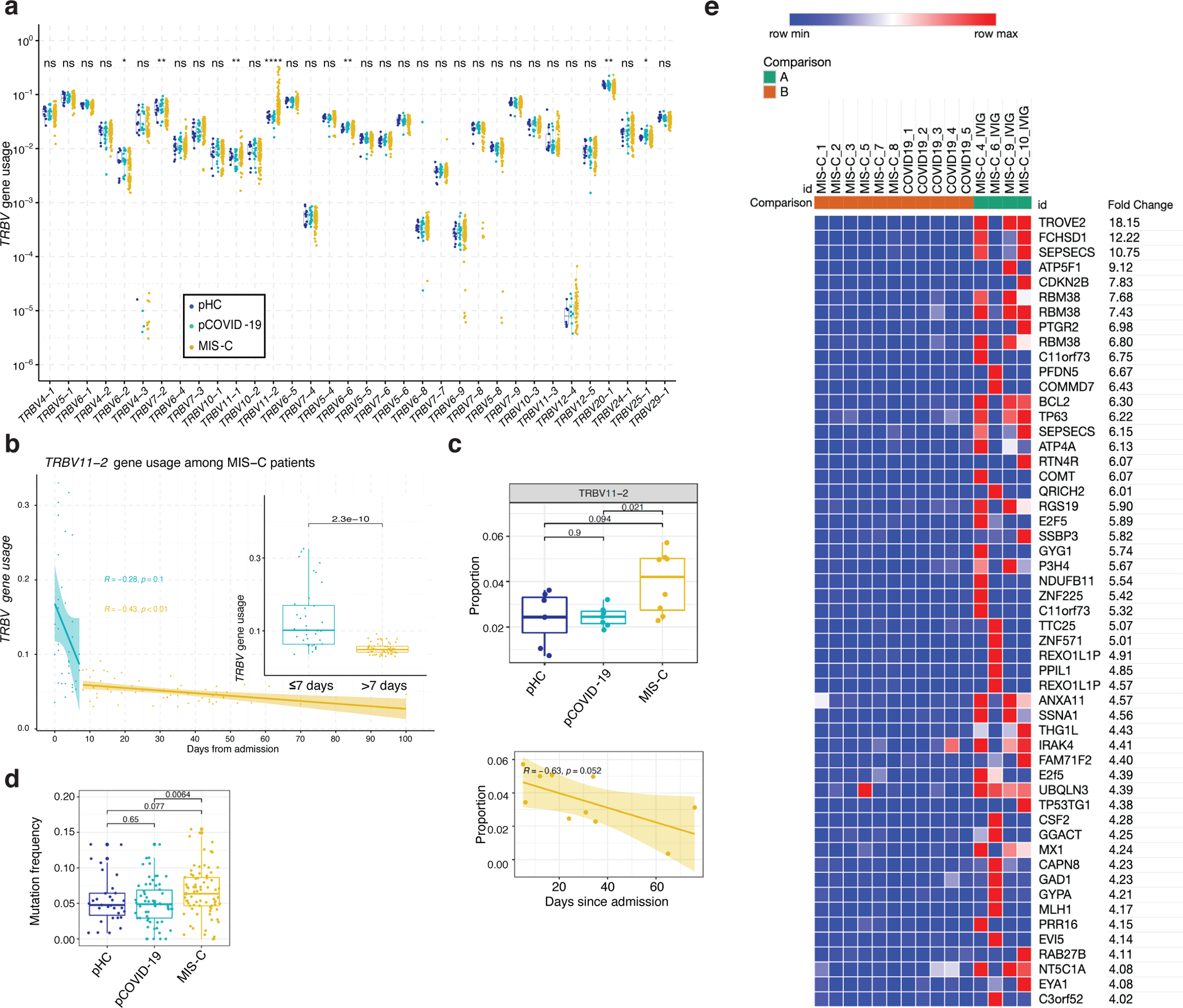
Pediatric Coronavirus Disease 2019 (pCOVID-19) is rarely severe; however, a minority of children infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) might develop multisystem inflammatory syndrome in children (MIS-C), with substantial morbidity. In this longitudinal multi-institutional study, we applied multi-omics (analysis of soluble biomarkers, proteomics, single-cell gene expression and immune repertoire analysis) to profile children with COVID-19 (n = 110) and MIS-C (n = 76), along with pediatric healthy controls (pHCs; n = 76). pCOVID-19 was characterized by robust type I interferon (IFN) responses, whereas prominent type II IFN-dependent and NF-κB-dependent signatures, matrisome activation and increased levels of circulating spike protein were detected in MIS-C, with no correlation with SARS-CoV-2 PCR status around the time of admission. Transient expansion of TRBV11-2 T cell clonotypes in MIS-C was associated with signatures of inflammation and T cell activation. The association of MIS-C with the combination of HLA A*02, B*35 and C*04 alleles suggests genetic susceptibility. MIS-C B cells showed higher mutation load than pCOVID-19 and pHC. These results identify distinct immunopathological signatures in pCOVID-19 and MIS-C that might help better define the pathophysiology of these disorders and guide therapy.
© 2022. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
Competing Interests Statement
TH and SH are employees and shareholders of CDI Laboratories. MA is a consultant for CDI Laboratories and the owner of Biomedical Hosting, LLC. TMS and IMK declare employment and equity ownership with Adaptive Biotechnologies. BAS is a former SomaLogic, Inc. (Boulder, CO, USA) employee and a company shareholder. The remaining authors declare no competing interests.
Figures

References
-
- Castagnoli R, et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents: A Systematic Review. JAMA Pediatr 174, 882–889 (2020). - PubMed
-
- CDC Health Advisory Panel. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19). Centers for Disease Control and Prevention. Available at https://emergency.cdc.gov/han/2020/han00432.asp. Accessed 28 June 2021.
Methods-only References
-
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available at https://www.covid19treatmentguidelines.nih.gov/. Accessed 28 June 2021. - PubMed
-
- Webtool For Basic Data Plotting And Analysis. An interactive open source software tool for a rapid first pass analysis. Available at https://foocheung.shinyapps.io/FFSv011/. Accessed on 01 July 2021.
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
