

A Systematic Review and Individual Patient Data Network Analysis of the Residual Symptom Structure Following Cognitive-Behavioral Therapy and Escitalopram, Mirtazapine and Venlafaxine for Depression
- PMID: 35178002
- PMCID: PMC8843824
- DOI: 10.3389/fpsyt.2022.746678
A Systematic Review and Individual Patient Data Network Analysis of the Residual Symptom Structure Following Cognitive-Behavioral Therapy and Escitalopram, Mirtazapine and Venlafaxine for Depression
Abstract
Objective: Consistent evidence suggests residual depressive symptomology are the strongest predictors of depression relapse following cognitive-behavioral therapy (CBT) and antidepressant medications (ADM's). Psychometric network models help detecting and understanding central symptoms that remain post-treatment, along with their complex co-occurrences. However, individual psychometric network studies show inconsistent findings. This systematic review and IPD network analysis aimed to estimate and compare the symptom network structures of residual depressive symptoms following CBT, ADM's, and their combination.
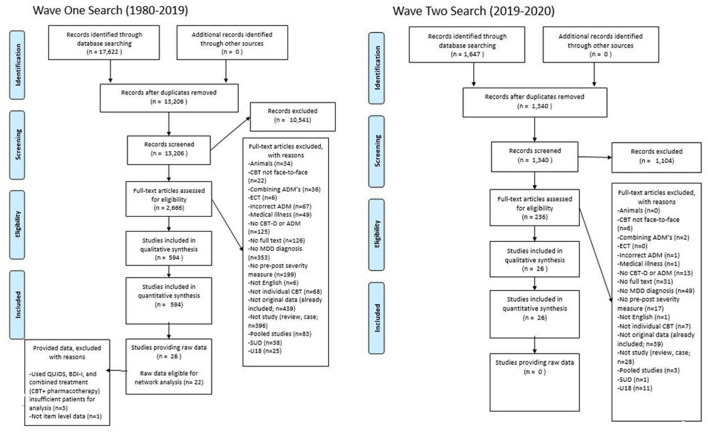
Methods: PsycINFO, PsycArticles, and PubMed were systematically searched through October 2020 for studies that have assessed individuals with major depression at post-treatment receiving either CBT and/or ADM's (venlafaxine, escitalopram, mirtazapine). IPD was requested from eligible samples to estimate and compare residual symptom psychometric network models post-CBT and post-ADM's.
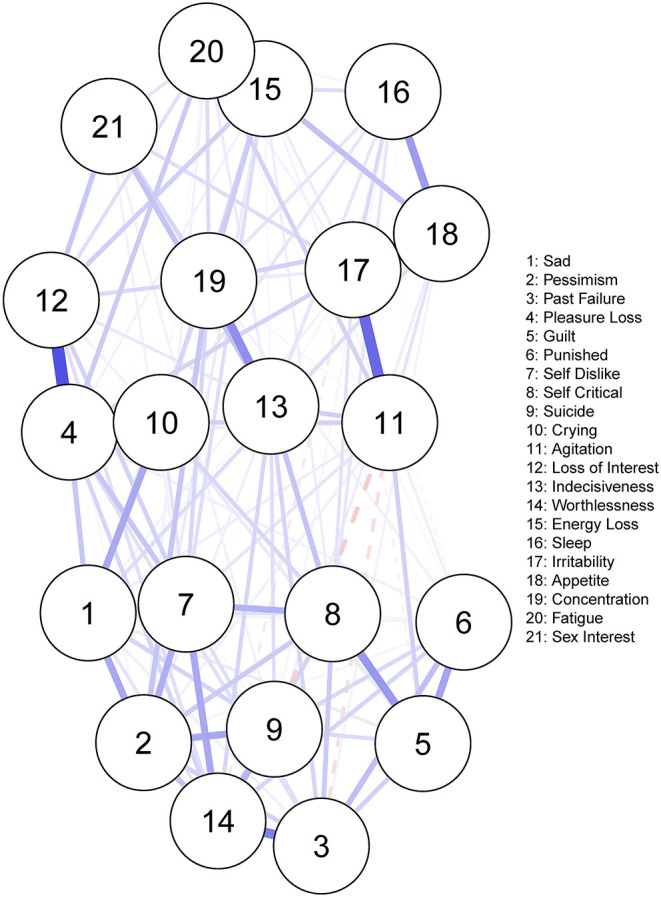
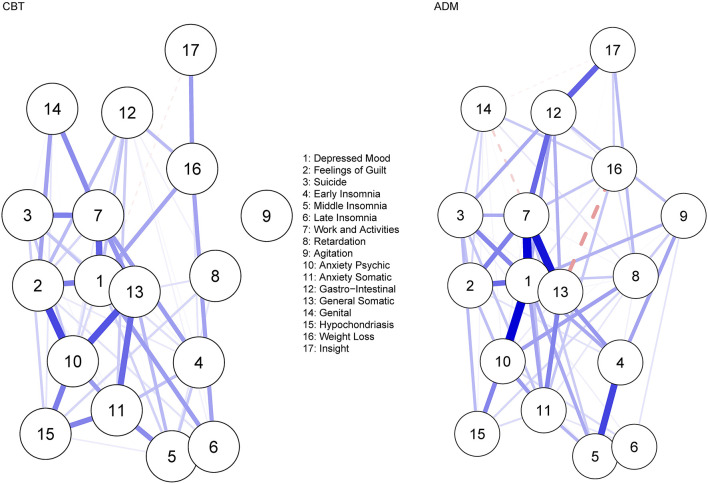
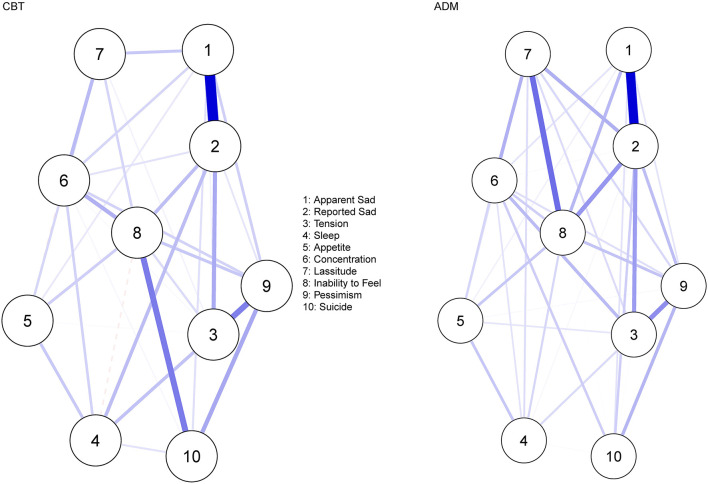
Results: In total, 25 from 663 eligible samples, including 1,389 patients qualified for the IPD. Depressed mood and anhedonia were consistently central residual symptoms post-CBT and post-ADM's. For CBT, fatigue-related and anxiety symptoms were also central post-treatment. A significant difference in network structure across treatments (CBT vs. ADM) was observed for samples measuring depression severity using the MADRS. Specifically, stronger symptom occurrences were present amongst lassitude-suicide post-CBT (vs. ADM's) and amongst lassitude-inability to feel post-ADM's (vs. CBT). No significant difference in global strength was observed across treatments.
Conclusions: Core major depression symptoms remain central across treatments, strategies to target these symptoms should be considered. Anxiety and fatigue related complaints also remain central post-CBT. Efforts must be made amongst researchers, institutions, and journals to permit sharing of IPD.Systematic Review Registration: A protocol was prospectively registered on PROSPERO (CRD42020141663; https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=141663).
Keywords: antidepressants; cognitive-behavioral therapy (CBT); depression; network psychometrics; residual symptomology.
Copyright © 2022 Whiston, Lennon, Brown, Looney, Larkin, O'Sullivan, Sik and Semkovska.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Rasmussen J, Young AH. Challenges of residual symptoms and functioning in management of MDD. Prog Neurol Psychiatry. (2018) 22:6–8. 10.1002/pnp.505 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources