

Clinical features and predictors of atrial fibrillation in patients with light-chain or transthyretin cardiac amyloidosis
- PMID: 35178887
- PMCID: PMC9065861
- DOI: 10.1002/ehf2.13851
Clinical features and predictors of atrial fibrillation in patients with light-chain or transthyretin cardiac amyloidosis
Abstract
Aims: The study aimed to investigate the prevalence, phenotypic characteristics, and predictors of atrial fibrillation (AF) in patients presenting with cardiac amyloidosis (CA) of light-chain (AL) or transthyretin (ATTR) type.
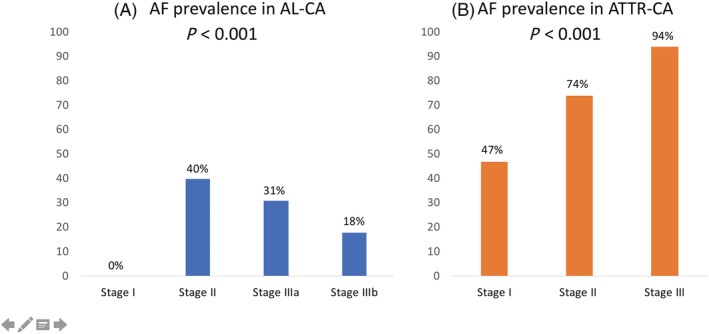
Methods and results: Clinical, biochemical, and echocardiographic data of patients presenting with CA between 2005 and 2020 were retrospectively collected. CA staging was based on established biomarker systems. Binomial logistic regression was run to analyse the effects of clinical variables on the likelihood of AF. The study included 133 patients [53% AL, 41% wild-type (wt) ATTR-CA, & 6% hereditary ATTR-CA]. Mean age was 71 years, and 80% were male patients. AF was diagnosed in 64 (48%) patients (28% in AL-CA, 80% in wtATTR, 13% in hATTR, P < 0.001). Patients with AF were older (74 vs. 69 years, P < 0.001), more likely to have wtATTR-CA (67 vs. 16%, P < 0.001), exhibited more often New York Heart Association ≥ III symptoms (66 vs. 45%, P = 0.02) and carried a higher burden of comorbidities. AF patients had lower left ventricular ejection fraction (47 vs. 53%, P < 0.005), higher left atrial volume index (54 vs. 46 mL/m2 , P = 0.007), higher pulmonary artery pressure (42 vs. 31 mmHg, P = 0.008), and worse tricuspid annular plane systolic excursion values (17 vs. 20 mm, P = 0.01). Mitral regurgitation ≥ Grade 2 was more frequent in AF (56 vs. 25%, P < 0.001). Higher ATTR-CA stage was associated with higher AF prevalence (47% vs. 74% vs. 94%, P < 0.001, for Stages I, II, & III, respectively). Higher AL-CA stage was associated with lower AF prevalence (0% vs. 40% vs. 31% vs. 18%, P < 0.001, for Stages I, II, IIIa, & IIIb, respectively). Three independent predictors for AF were identified in a multivariate logistic regression model with 81.5% classification accuracy: AL type [odds ratio (OR) 0.1, confidence interval (CI) 0.01-0.29, P = 0.001], estimated glomerular filtration rate (OR 0.9, CI 0.93-0.99, P = 0.03), and body mass index (OR 1.3, CI 1.07-1.66, P = 0.01). ATTR amyloidosis was associated with a 10-fold higher risk of AF. During 1 year follow-up, only one episode of ischaemic stroke was reported.
Conclusions: Atrial fibrillation affects nearly half of all patients with CA. Patients presenting with AF have more severe symptoms and higher burden of comorbidities. ATTR type of amyloidosis is the strongest predictor of AF. Prospective screening for occult AF may be considered in ATTR-CA.
Keywords: Amyloidosis; Atrial fibrillation; Cardiomyopathy; Light-chain; Transthyretin.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- González‐López E, Gallego‐Delgado M, Guzzo‐Merello G, de Haro‐del Moral FJ, Cobo‐Marcos M, Robles C, Bornstein B, Salas C, Lara‐Pezzi E, Alonso‐Pulpon L, Garcia‐Pavia P. Wild‐type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur Heart J 2015; 36: 2585–2594. - PubMed
-
- Hahn VS, Yanek LR, Vaishnav J, Ying W, Vaidya D, Lee YZJ, Riley SJ, Subramanya V, Brown EE, Hopkins CD, Ononogbu S, Perzel Mandell K, Halushka MK, Steenbergen C Jr, Rosenberg AZ, Tedford RJ, Judge DP, Shah SJ, Russell SD, Kass DA, Sharma K. Endomyocardial biopsy characterization of heart failure with preserved ejection fraction and prevalence of cardiac amyloidosis. JACC Hear Fail 2020; 8: 712–724. - PMC - PubMed
-
- Treibel TA, Fontana M, Gilbertson JA, Castelletti S, White SK, Scully PR, Roberts N, Hutt DF, Rowczenio DM, Whelan CJ, Ashworth MA, Gillmore JD, Hawkins PN, Moon JC. Occult transthyretin cardiac amyloid in severe calcific aortic stenosis. Circ Cardiovasc Imaging 2016; 9: 1–10. - PubMed
-
- Castano A, Narotsky DL, Hamid N, Khalique OK, Morgenstern R, DeLuca A, Rubin J, Chiuzan C, Nazif T, Vahl T, George I. Unveiling transthyretin cardiac amyloidosis and its predictors among elderly patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur Heart J 2017; 38: 2879–2887. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
