

Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer
- PMID: 35179323
- PMCID: PMC9844551
- DOI: 10.1056/NEJMoa2119115
Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer
Abstract
Background: Darolutamide is a potent androgen-receptor inhibitor that has been associated with increased overall survival among patients with nonmetastatic, castration-resistant prostate cancer. Whether a combination of darolutamide, androgen-deprivation therapy, and docetaxel would increase survival among patients with metastatic, hormone-sensitive prostate cancer is unknown.
Methods: In this international, phase 3 trial, we randomly assigned patients with metastatic, hormone-sensitive prostate cancer in a 1:1 ratio to receive darolutamide (at a dose of 600 mg [two 300-mg tablets] twice daily) or matching placebo, both in combination with androgen-deprivation therapy and docetaxel. The primary end point was overall survival.
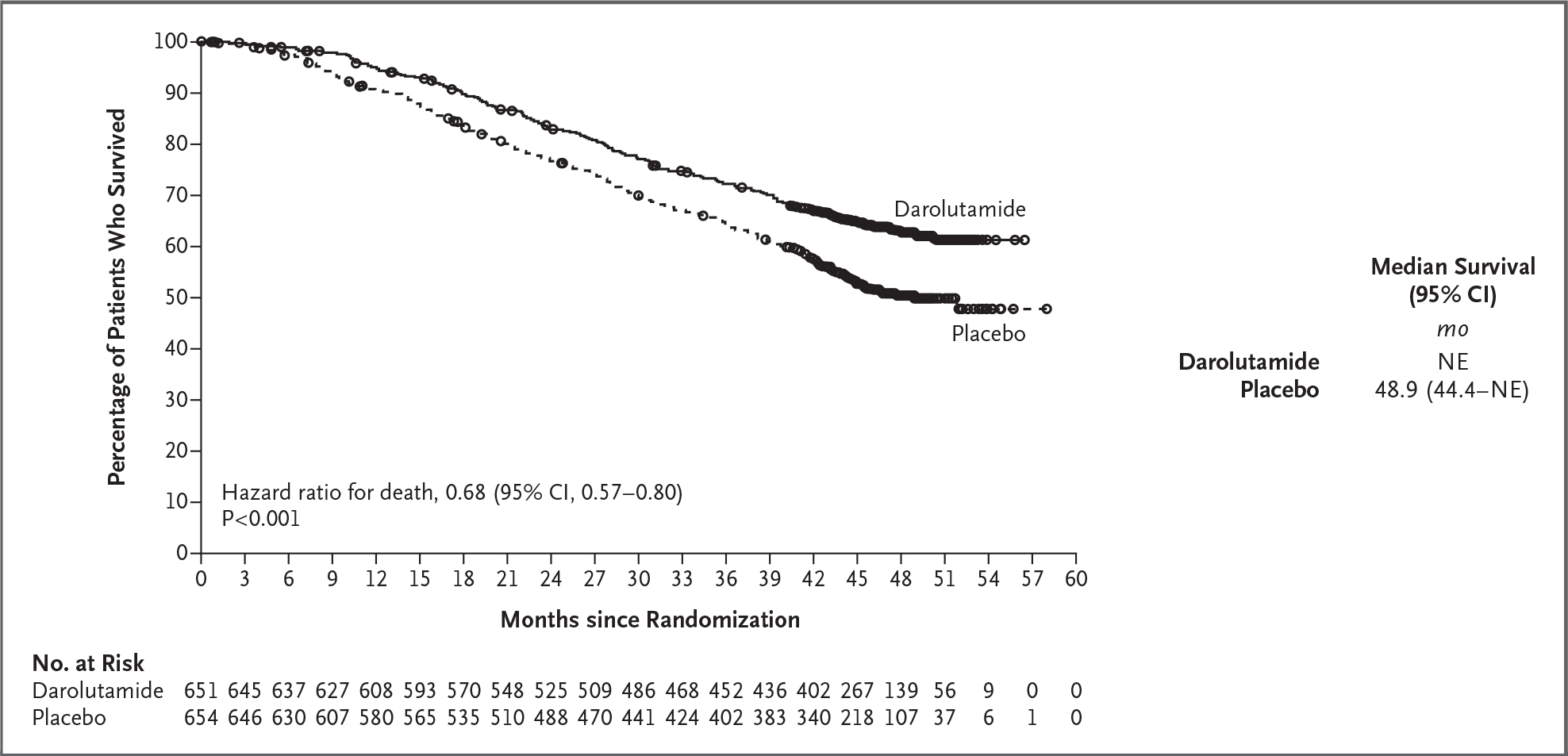
Results: The primary analysis involved 1306 patients (651 in the darolutamide group and 655 in the placebo group); 86.1% of the patients had disease that was metastatic at the time of the initial diagnosis. At the data cutoff date for the primary analysis (October 25, 2021), the risk of death was significantly lower, by 32.5%, in the darolutamide group than in the placebo group (hazard ratio 0.68; 95% confidence interval, 0.57 to 0.80; P<0.001). Darolutamide was also associated with consistent benefits with respect to the secondary end points and prespecified subgroups. Adverse events were similar in the two groups, and the incidences of the most common adverse events (occurring in ≥10% of the patients) were highest during the overlapping docetaxel treatment period in both groups. The frequency of grade 3 or 4 adverse events was 66.1% in the darolutamide group and 63.5% in the placebo group; neutropenia was the most common grade 3 or 4 adverse event (in 33.7% and 34.2%, respectively).
Conclusions: In this trial involving patients with metastatic, hormone-sensitive prostate cancer, overall survival was significantly longer with the combination of darolutamide, androgen-deprivation therapy, and docetaxel than with placebo plus androgen-deprivation therapy and docetaxel, and the addition of darolutamide led to improvement in key secondary end points. The frequency of adverse events was similar in the two groups. (Funded by Bayer and Orion Pharma; ARASENS ClinicalTrials.gov number, NCT02799602.).
Copyright © 2022 Massachusetts Medical Society.
Figures

Comment in
-
Darolutamide combo is an ARASENSible option for mHSPC.Nat Rev Urol. 2022 Apr;19(4):194. doi: 10.1038/s41585-022-00579-0. Nat Rev Urol. 2022. PMID: 35236955 No abstract available.
-
Darolutamide combo is a sensible option for mHSPC.Nat Rev Clin Oncol. 2022 Apr;19(4):219. doi: 10.1038/s41571-022-00616-2. Nat Rev Clin Oncol. 2022. PMID: 35260806 No abstract available.
-
Urological Oncology: Prostate Cancer.J Urol. 2022 Jul;208(1):214-216. doi: 10.1097/JU.0000000000002705. Epub 2022 Apr 25. J Urol. 2022. PMID: 35467383 No abstract available.
-
Darolutamide and survival in metastatic, hormone-sensitive prostate cancer: a patient and caregiver perspective and plain language summary of the ARASENS trial.Future Oncol. 2022 Jul;18(21):2585-2597. doi: 10.2217/fon-2022-0433. Epub 2022 Jun 3. Future Oncol. 2022. PMID: 35656777
-
Darolutamide in Metastatic Prostate Cancer.N Engl J Med. 2022 Jun 16;386(24):2344. doi: 10.1056/NEJMc2205310. N Engl J Med. 2022. PMID: 35704492 No abstract available.
-
Darolutamide in Metastatic Prostate Cancer.N Engl J Med. 2022 Jun 16;386(24):2344. doi: 10.1056/NEJMc2205310. N Engl J Med. 2022. PMID: 35704493 No abstract available.
References
-
- Gillessen S, Attard G, Beer TM, et al. Management of patients with advanced prostate cancer: report of the Advanced Prostate Cancer Consensus Conference 2019. Eur Urol 2020;77:508–47. - PubMed
-
- Lowrance W, Breau R, Chou R, et al. Advanced prostate cancer: AUA/ASTRO/SUO guideline. American Urological Association, 2020. (https://www.auanet.org/documents/Guidelines/PDF/Advanced%20Prostate%20Ca...).
-
- Mottet N, Cornford P, van den Bergh RCN, et al. Guidelines on prostate cancer. European Associated of Urology, 2021. (https://uroweb.org/guideline/prostate-cancer/). - PubMed
-
- Parker C, Castro E, Fizazi K, et al. Prostate cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 2020;31:1119–34. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical