

Association of Positive End-Expiratory Pressure and Lung Recruitment Selection Strategies with Mortality in Acute Respiratory Distress Syndrome: A Systematic Review and Network Meta-analysis
- PMID: 35180042
- PMCID: PMC12042658
- DOI: 10.1164/rccm.202108-1972OC
Association of Positive End-Expiratory Pressure and Lung Recruitment Selection Strategies with Mortality in Acute Respiratory Distress Syndrome: A Systematic Review and Network Meta-analysis
Abstract
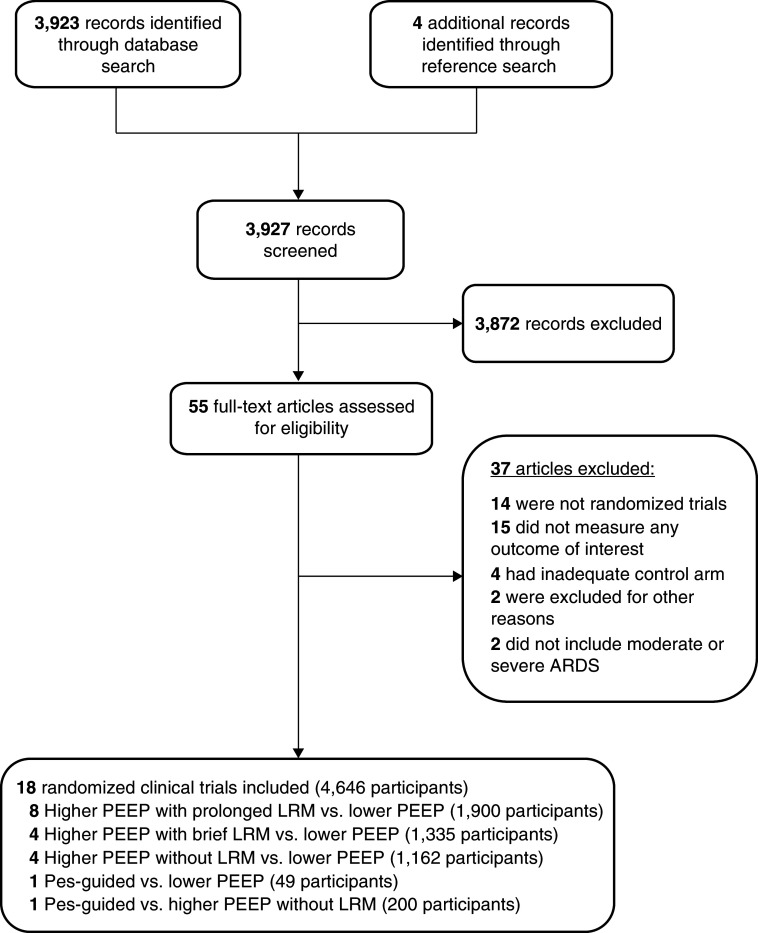
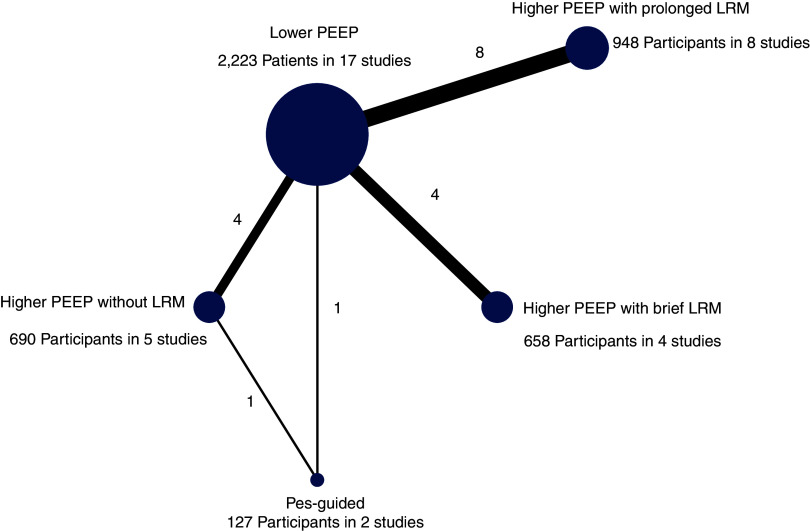
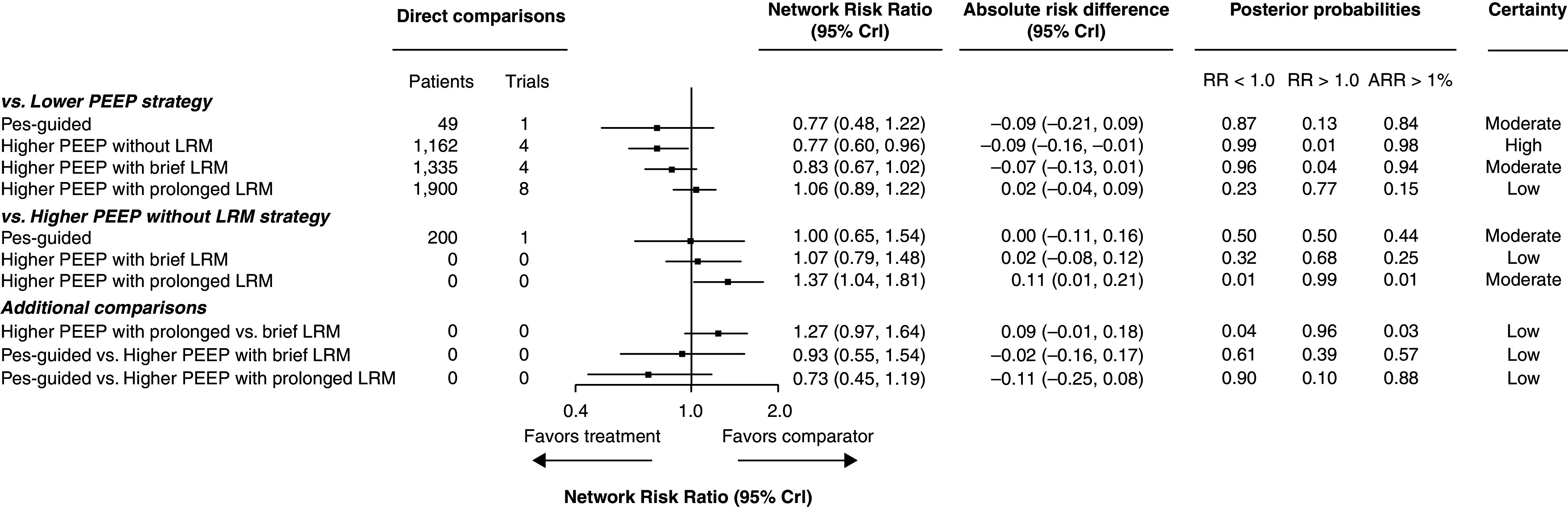
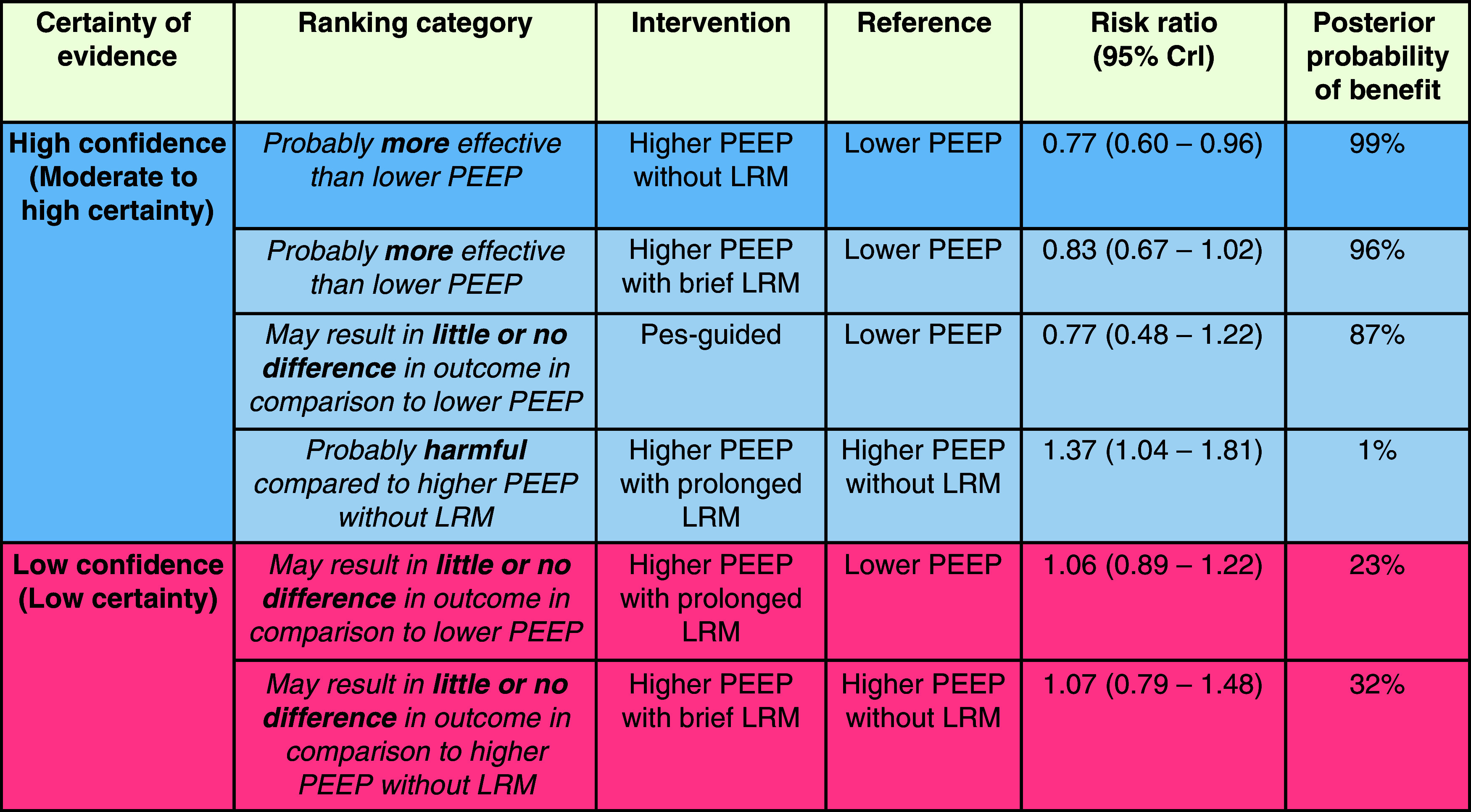
Rationale: The most beneficial positive end-expiratory pressure (PEEP) selection strategy in patients with acute respiratory distress syndrome (ARDS) is unknown, and current practice is variable. Objectives: To compare the relative effects of different PEEP selection strategies on mortality in adults with moderate to severe ARDS. Methods: We conducted a network meta-analysis using a Bayesian framework. Certainty of evidence was evaluated using grading of recommendations assessment, development and evaluation methodology. Measurements and Main Results: We included 18 randomized trials (4,646 participants). Compared with a lower PEEP strategy, the posterior probability of mortality benefit from a higher PEEP without lung recruitment maneuver (LRM) strategy was 99% (risk ratio [RR], 0.77; 95% credible interval [CrI], 0.60-0.96, high certainty), the posterior probability of benefit of the esophageal pressure-guided strategy was 87% (RR, 0.77; 95% CrI, 0.48-1.22, moderate certainty), the posterior probability of benefit of a higher PEEP with brief LRM strategy was 96% (RR, 0.83; 95% CrI, 0.67-1.02, moderate certainty), and the posterior probability of increased mortality from a higher PEEP with prolonged LRM strategy was 77% (RR, 1.06; 95% CrI, 0.89-1.22, low certainty). Compared with a higher PEEP without LRM strategy, the posterior probability of increased mortality from a higher PEEP with prolonged LRM strategy was 99% (RR, 1.37; 95% CrI, 1.04-1.81, moderate certainty). Conclusions: In patients with moderate to severe ARDS, higher PEEP without LRM is associated with a lower risk of death than lower PEEP. A higher PEEP with prolonged LRM strategy is associated with increased risk of death when compared with higher PEEP without LRM.
Keywords: ARDS; PEEP; hypoxemic respiratory failure; lung recruitment maneuver; mortality.
Figures
Comment in
-
High Positive End-Expiratory Pressure and Lung Recruitment in Moderate to Severe Acute Respiratory Distress Syndrome: Does One Size Really Fit All?Am J Respir Crit Care Med. 2022 Jun 1;205(11):1260-1262. doi: 10.1164/rccm.202202-0281ED. Am J Respir Crit Care Med. 2022. PMID: 35297740 Free PMC article. No abstract available.
References
-
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. American Thoracic Society, European Society of Intensive Care Medicine, and Society of Critical Care Medicine An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med . 2017;195:1253–1263. - PubMed
-
- Webb HH, Tierney DF. Experimental pulmonary edema due to intermittent positive pressure ventilation with high inflation pressures: protection by positive end-expiratory pressure. Am Rev Respir Dis . 1974;110:556–565. - PubMed
-
- Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med . 2013;369:2126–2136. - PubMed
-
- Del Sorbo L, Tonetti T, Ranieri VM. Alveolar recruitment in acute respiratory distress syndrome: should we open the lung (no matter what) or may accept (part of) the lung closed? Intensive Care Med . 2019;45:1436–1439. - PubMed
-
- Gattinoni L, Carlesso E, Cressoni M. Selecting the ‘right’ positive end-expiratory pressure level. Curr Opin Crit Care . 2015;21:50–57. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
