

Follicular Lymphoma: a Focus on Current and Emerging Therapies
- PMID: 35180337
- PMCID: PMC9329020
- DOI: 10.46883/2022.25920946
Follicular Lymphoma: a Focus on Current and Emerging Therapies
Abstract
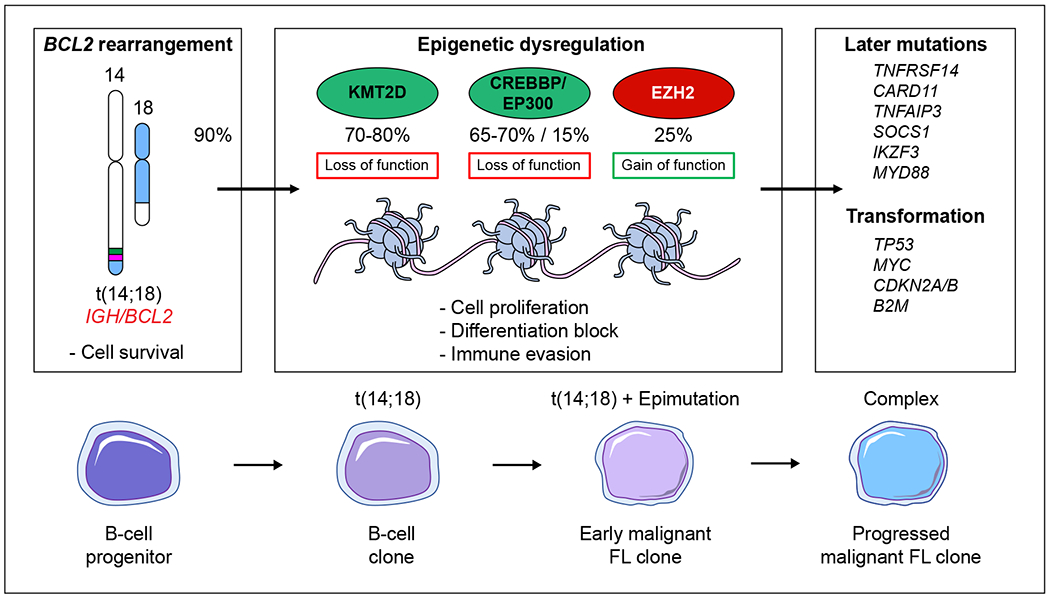
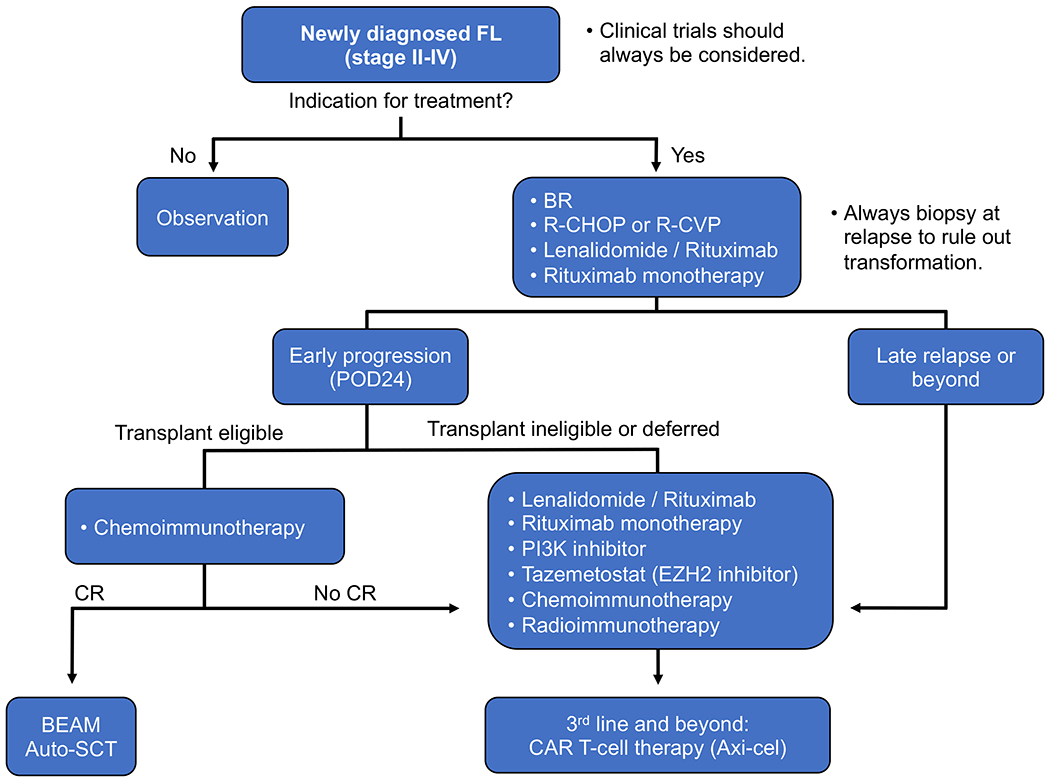
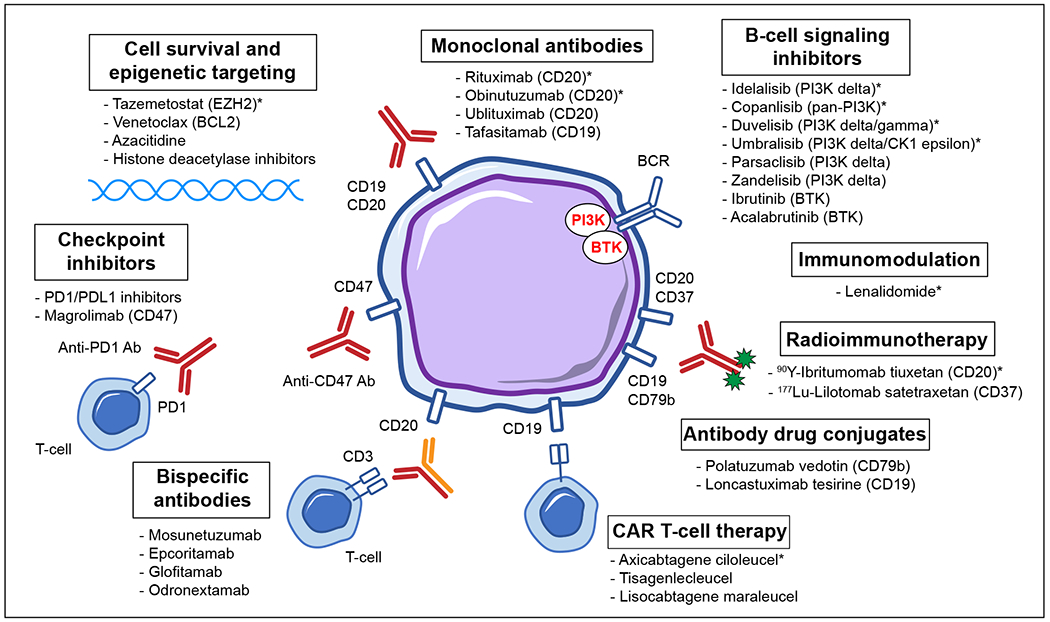
Follicular lymphoma (FL) is the most common indolent lymphoma and is characterized by a relapsing and remitting course. In addition to significant biologic heterogeneity, the clinical trajectory for patients is variable, with some being observed for many years, and others having aggressive disease requiring multiple treatment courses. Unfortunately, FL remains incurable, and continues to cause early mortality. Improved understanding of the genetic and immune biology of FL has led to several FDA-approved therapies in the relapsed and refractory setting, including PI3K inhibitors; immunomodulatory agents; the EZH2 inhibitor, tazemetostat; and anti-CD19 chimeric antigen receptor (CAR) T-cell therapy, axicabtagene ciloleucel. This review outlines the current approach to the diagnosis and treatment of FL with a focus on emerging investigational therapies, including targeted protein inhibitors, antibody-drug conjugates, monoclonal antibodies, bispecific antibodies, and novel combination strategies.
Figures
References
-
- Link BK, Maurer MJ, Nowakowski GS, et al. Rates and outcomes of follicular lymphoma transformation in the immunochemotherapy era: a report from the University of Iowa/MayoClinic Specialized Program of Research Excellence Molecular Epidemiology Resource. J Clin Oncol. 2013;31(26):3272–3278. doi: 10.1200/JCO.2012.48.3990 - DOI - PMC - PubMed
-
- Casulo C, Byrtek M, Dawson KL, et al. Early relapse of follicular lymphoma after rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone defines patients at high risk for death: an analysis from the National LymphoCare Study. J Clin Oncol. 2015;33(23):2516–2522. doi: 10.1200/JCO.2014.59.7534 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
