

Clinical Subtypes of Sepsis Survivors Predict Readmission and Mortality after Hospital Discharge
- PMID: 35180373
- PMCID: PMC9353958
- DOI: 10.1513/AnnalsATS.202109-1088OC
Clinical Subtypes of Sepsis Survivors Predict Readmission and Mortality after Hospital Discharge
Abstract
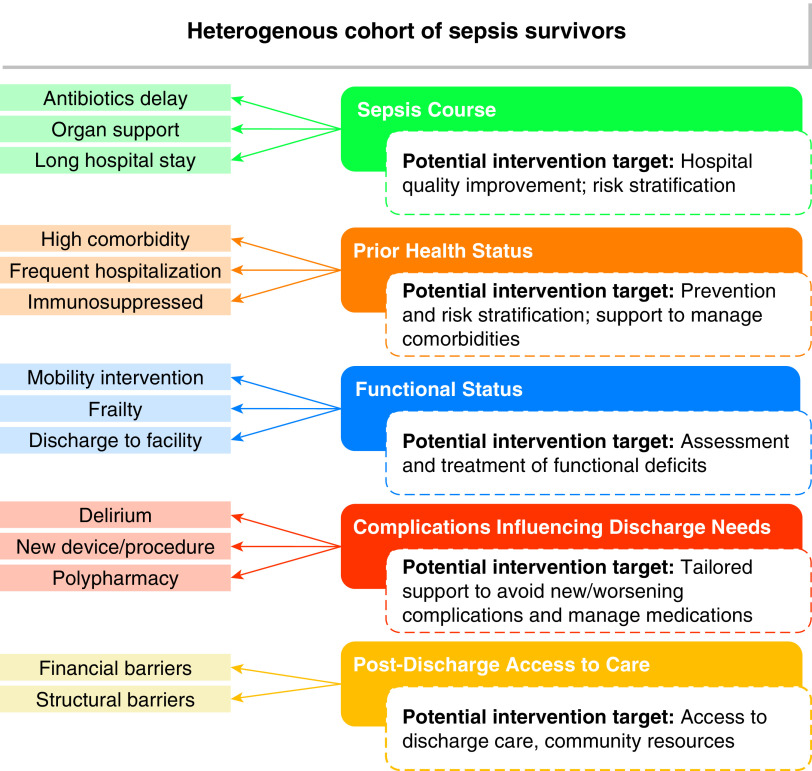
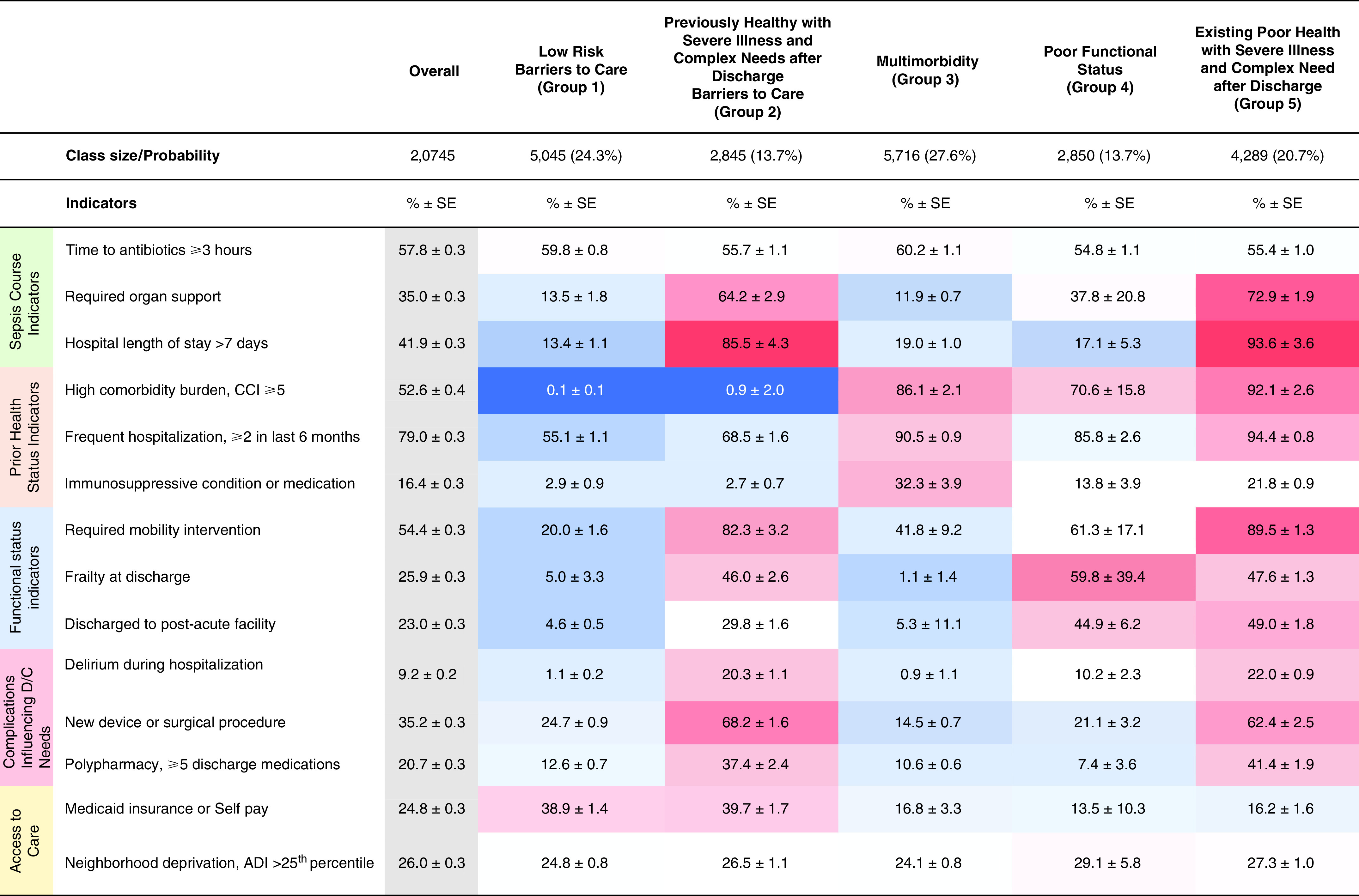
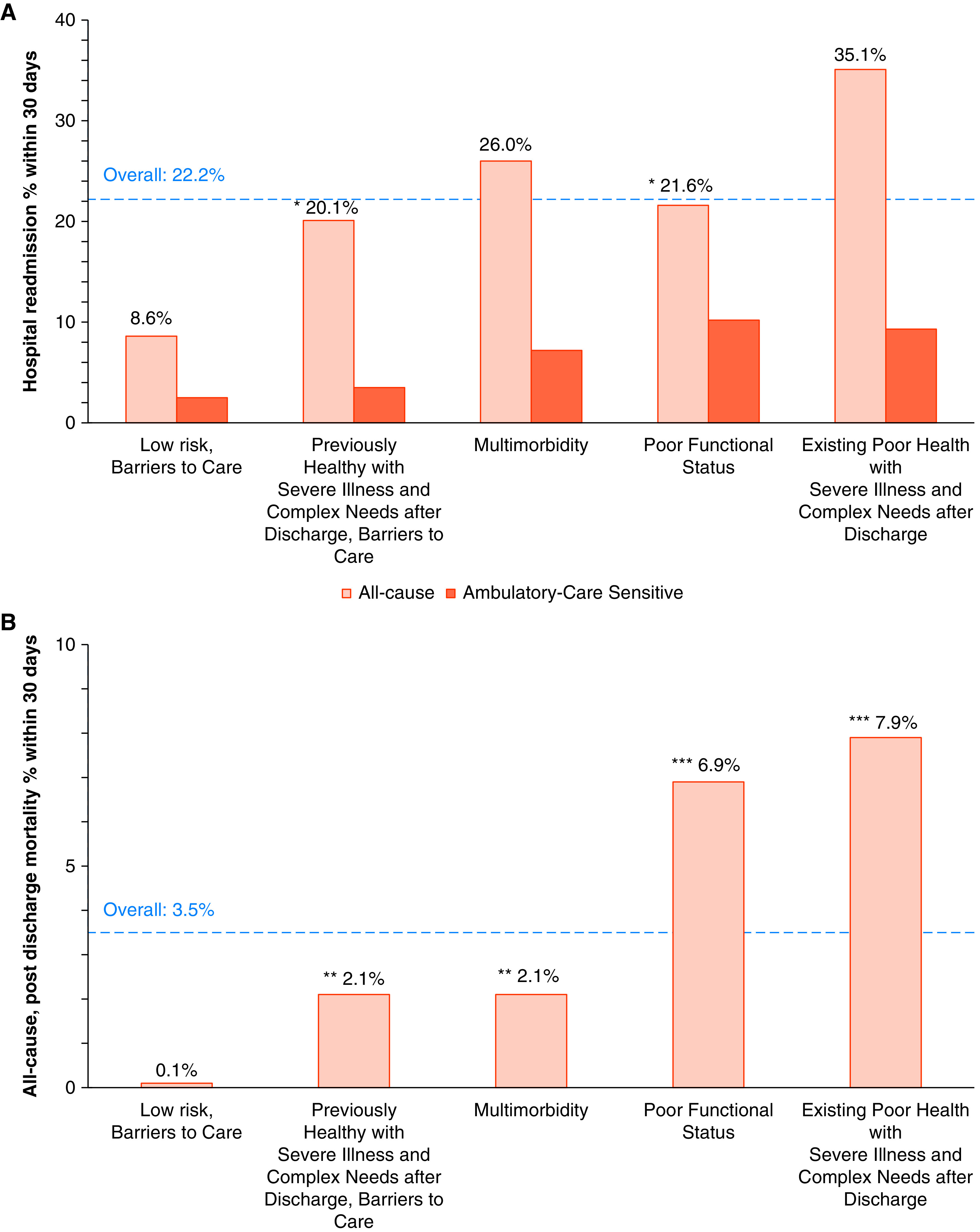
Rationale: Sepsis survivors experience adverse outcomes including high rates of postdischarge mortality and rehospitalization. Given the heterogeneity of the condition, using a person-centered framework to identify subtypes within this population with different risks of postdischarge outcomes may optimize postsepsis care. Objectives: To classify individuals into subtypes and assess the association of subtypes with 30-day rehospitalization and mortality. Methods: We conducted a retrospective observational study between January 2014 and October 2017 among 20,745 patients admitted to one of 12 southeastern U.S. hospitals with a clinical definition of sepsis. We used latent class analysis to classify sepsis survivors into subtypes, which were evaluated against 30-day readmission and mortality rates using a specialized regression approach. A secondary analysis evaluated subtypes against readmission rate for ambulatory care-sensitive conditions. Results: Among 20,745 patients, latent class analysis identified five distinct subtypes as the optimal solution. Clinical subtype was associated with 30-day readmission, with the subtype existing poor health with severe illness and complex needs after discharge demonstrating highest risk (35%) and the subtype low risk, barriers to care demonstrating the lowest risk (9%). Forty-seven percent of readmissions in the subtype poor functional status were for ambulatory care-sensitive conditions, whereas 17% of readmissions in the subtype previously healthy with severe illness and complex needs after discharge, barriers to care were for ambulatory care-sensitive conditions. Subtype was significantly associated with 30-day mortality: highest in for existing poor health with severe illness and complex needs after discharge (8%) and lowest for low risk, barriers to care (0.1%). Conclusions: Sepsis survivors can be classified into subtypes representing nuanced constellations of characteristics, with differential 30-day mortality and readmission risk profiles. Predischarge classification may allow an individualized approach to postsepsis care.
Keywords: hospital readmission; mortality; phenotype; sepsis; survivor.
Figures
Comment in
-
Toward Tailored Care for Sepsis Survivors.Ann Am Thorac Soc. 2022 Aug;19(8):1271-1272. doi: 10.1513/AnnalsATS.202203-240ED. Ann Am Thorac Soc. 2022. PMID: 35913466 Free PMC article. No abstract available.
References
-
- Fleischmann C, Scherag A, Adhikari NKJ, Hartog CS, Tsaganos T, Schlattmann P, et al. International Forum of Acute Care Trialists Assessment of global incidence and mortality of hospital-treated sepsis: current estimates and limitations. Am J Respir Crit Care Med . 2016;193:259–272. - PubMed
-
- Mayr FB, Talisa VB, Balakumar V, Chang CH, Fine M, Yende S. Proportion and cost of unplanned 30-day readmissions after sepsis compared with other medical conditions. JAMA . 2017;317:530–531. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
