

Use of statins for the prevention of cardiovascular disease in 41 low-income and middle-income countries: a cross-sectional study of nationally representative, individual-level data
- PMID: 35180420
- PMCID: PMC8896912
- DOI: 10.1016/S2214-109X(21)00551-9
Use of statins for the prevention of cardiovascular disease in 41 low-income and middle-income countries: a cross-sectional study of nationally representative, individual-level data
Abstract
Background: In the prevention of cardiovascular disease, a WHO target is that at least 50% of eligible people use statins. Robust evidence is needed to monitor progress towards this target in low-income and middle-income countries (LMICs), where most cardiovascular disease deaths occur. The objectives of this study were to benchmark statin use in LMICs and to investigate country-level and individual-level characteristics associated with statin use.
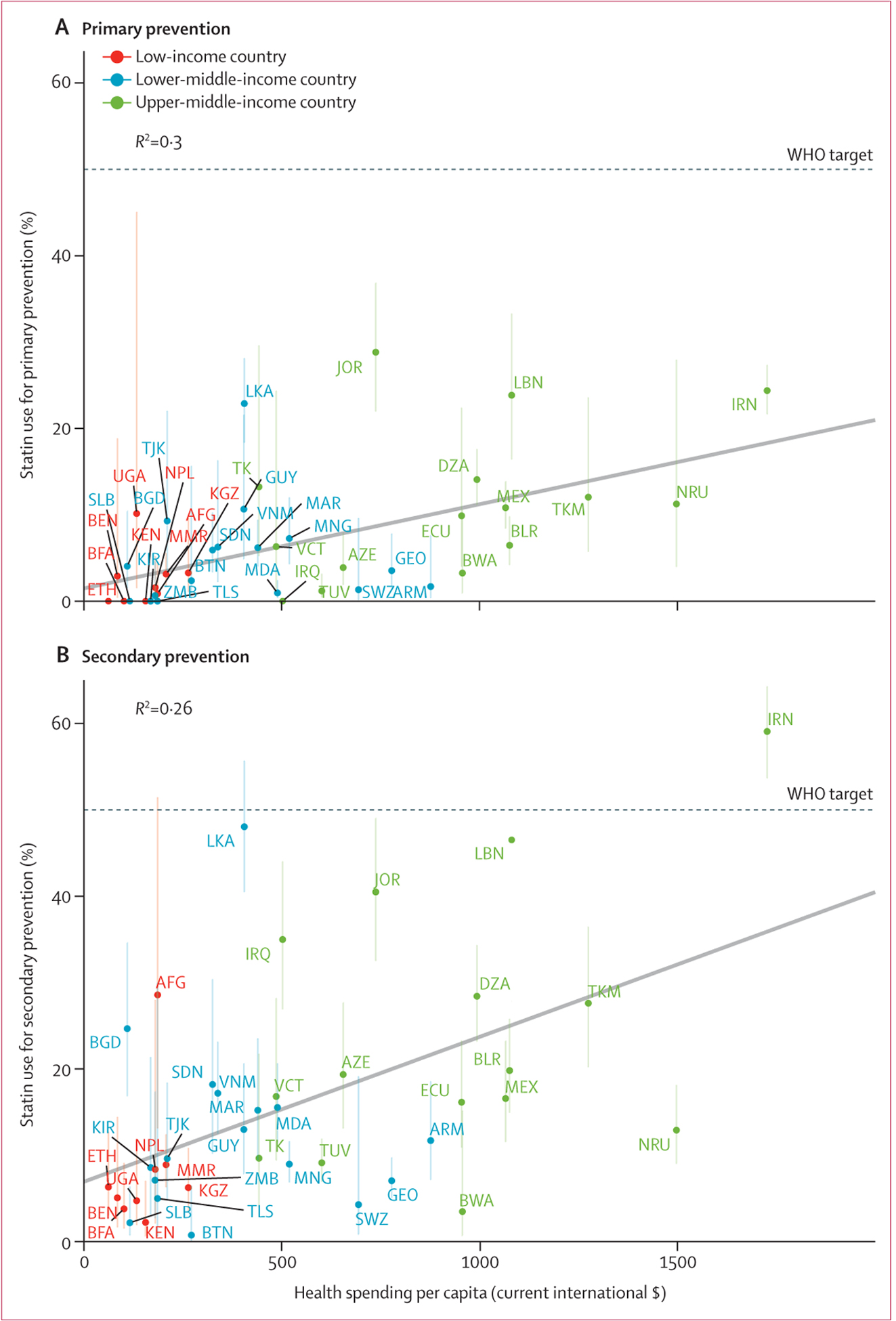
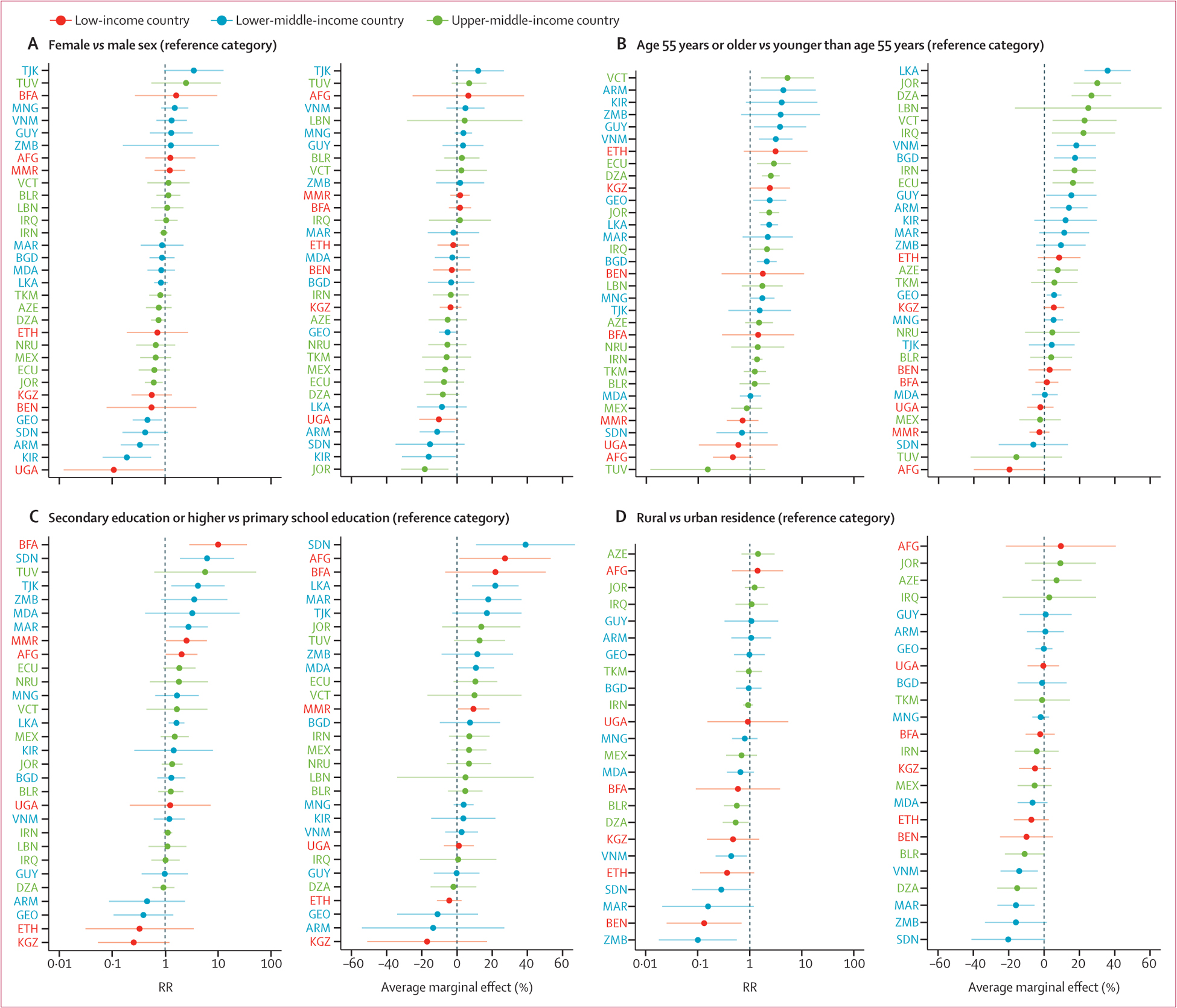
Methods: We did a cross-sectional analysis of pooled, individual-level data from nationally representative health surveys done in 41 LMICs between 2013 and 2019. Our sample consisted of non-pregnant adults aged 40-69 years. We prioritised WHO Stepwise Approach to Surveillance (STEPS) surveys because these are WHO's recommended method for population monitoring of non-communicable disease targets. For countries in which no STEPS survey was available, a systematic search was done to identify other surveys. We included surveys that were done in an LMIC as classified by the World Bank in the survey year; were done in 2013 or later; were nationally representative; had individual-level data available; and asked questions on statin use and previous history of cardiovascular disease. Primary outcomes were the proportion of eligible individuals self-reporting use of statins for the primary and secondary prevention of cardiovascular disease. Eligibility for statin therapy for primary prevention was defined among individuals with a history of diagnosed diabetes or a 10-year cardiovascular disease risk of at least 20%. Eligibility for statin therapy for secondary prevention was defined among individuals with a history of self-reported cardiovascular disease. At the country level, we estimated statin use by per-capita health spending, per-capita income, burden of cardiovascular diseases, and commitment to non-communicable disease policy. At the individual level, we used modified Poisson regression models to assess statin use alongside individual-level characteristics of age, sex, education, and rural versus urban residence. Countries were weighted in proportion to their population size in pooled analyses.
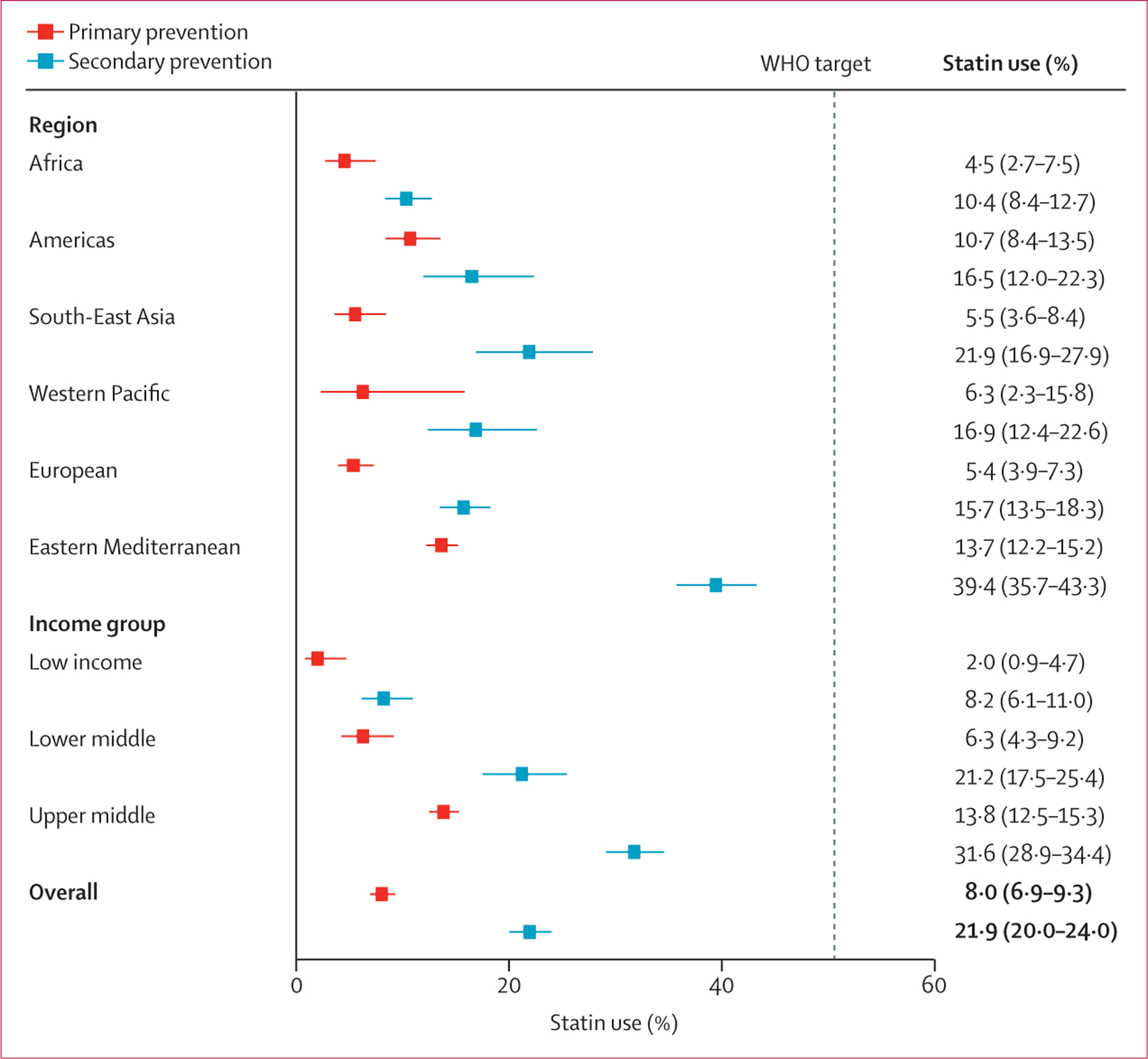
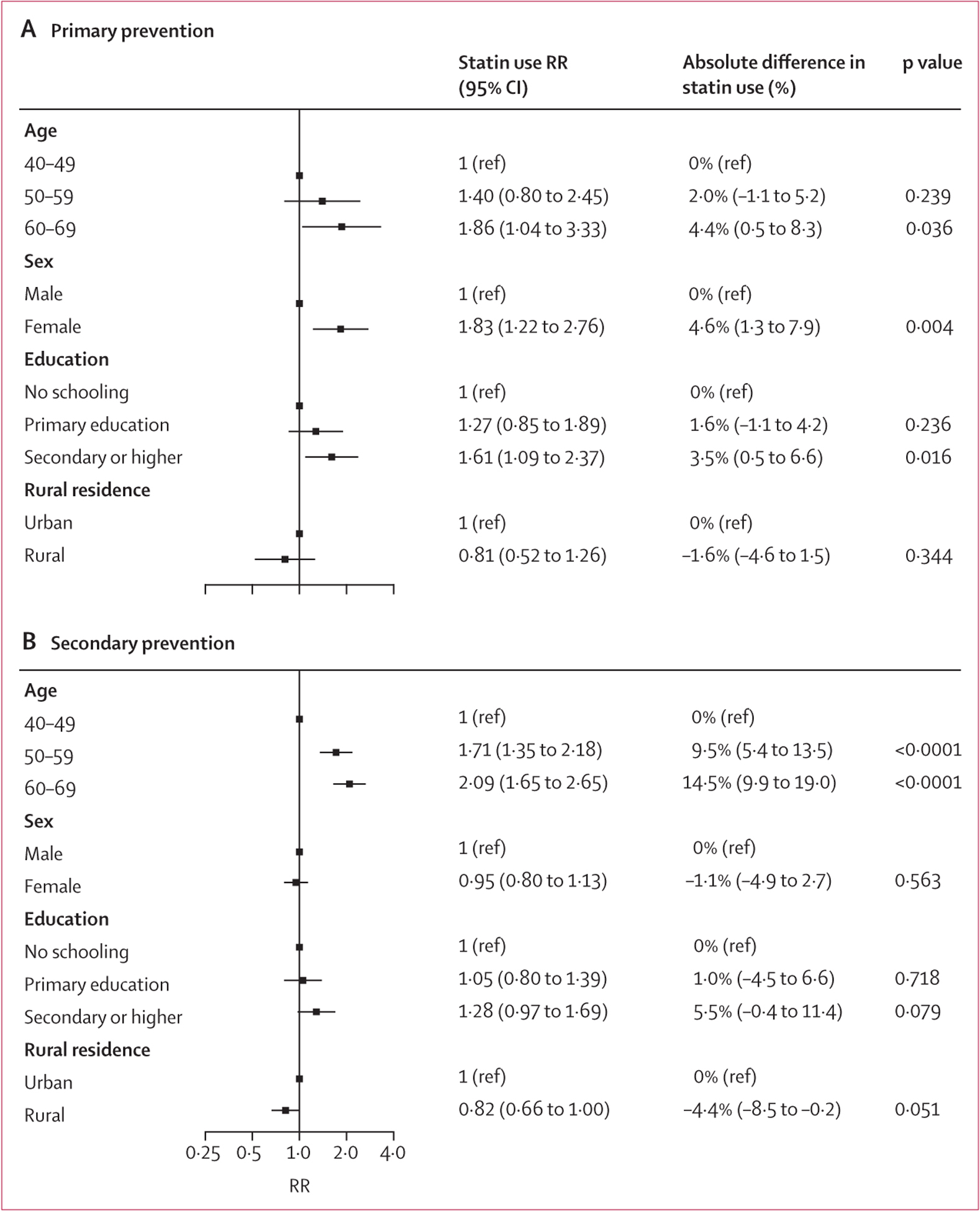
Findings: The final pooled sample included 116 449 non-pregnant individuals. 9229 individuals reported a previous history of cardiovascular disease (7·9% [95% CI 7·4-8·3] of the population-weighted sample). Among those without a previous history of cardiovascular disease, 8453 were eligible for a statin for primary prevention of cardiovascular disease (9·7% [95% CI 9·3-10·1] of the population-weighted sample). For primary prevention of cardiovascular disease, statin use was 8·0% (95% CI 6·9-9·3) and for secondary prevention statin use was 21·9% (20·0-24·0). The WHO target that at least 50% of eligible individuals receive statin therapy to prevent cardiovascular disease was achieved by no region or income group. Statin use was less common in countries with lower health spending. At the individual level, there was generally higher statin use among women (primary prevention only, risk ratio [RR] 1·83 [95% CI 1·22-2·76), and individuals who were older (primary prevention, 60-69 years, RR 1·86 [1·04-3·33]; secondary prevention, 50-59 years RR 1·71 [1·35-2·18]; and 60-69 years RR 2·09 [1·65-2·65]), more educated (primary prevention, RR 1·61 [1·09-2·37]; secondary prevention, RR 1·28 [0·97-1·69]), and lived in urban areas (secondary prevention only, RR 0·82 [0·66-1·00]).
Interpretation: In a diverse sample of LMICs, statins are used by about one in ten eligible people for the primary prevention of cardiovascular diseases and one in five eligible people for secondary prevention. There is an urgent need to scale up statin use in LMICs to achieve WHO targets. Policies and programmes that facilitate implementation of statins into primary health systems in these settings should be investigated for the future.
Funding: National Clinician Scholars Program at the University of Michigan Institute for Healthcare Policy and Innovation, and National Institute of Diabetes and Digestive and Kidney Diseases.
Translation: For the Spanish translation of the abstract see Supplementary Materials section.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests JML reports graduate research funding from the German Academic Scholarship Foundation. RA reports contracts with Novo Nordisk, Union for International Cancer Control's, National Institute for Health Research, and Sloan Memorial Kettering Hospital, outside of the submitted work. RA also reports payments or honoraria from Merck, Novartis, and F Hoffmann-La Roche, outside of the submitted work. TWB reports support from the Alexander von Humboldt Foundation. MH reports grants from the National Institutes of Health and receives salary support from Physician for Human Rights. MDH received funding in the past 3 years from the World Heart Federation to serve as its senior programme advisor for the Emerging Leaders programme, which has been supported by Boehringer Ingelheim, Novartis, Bupa, and AstraZeneca. MDH also received support from the American Heart Association, Verily, AstraZeneca, and American Medical Association for work unrelated to this research. MDH plans to submit patents for heart failure polypill. MDH has received meeting or travel support from the American Heart Association and World Heart Federation. MDH has an appointment at The George Institute for Global Health, which has a patent, licence, and has received investment funding with intent to commercialise fixed-dose combination therapy through its social enterprise business, George Medicines. DF reports grant funding within the past 3 years from a Pilot and Feasibility Grant funded by the Michigan Center for Diabetes Translational Research (NIH Grant P30-DK092926) and a grant from the Swinmurn Foundation to implement a sustainable diabetes clinic in Guatemala. DF also reports volunteer affiliations with Wuqu’ Kawoq and GlucoSalud, outside of the submitted work. During the course of this study, DF has received research fellowship funding from National Clinician Scholars Program at the University of Michigan Institute for Healthcare Policy & Innovation. All other authors declare no competing interests.
Figures
Comment in
-
Statins: are they appropriate for all patients?Lancet Glob Health. 2022 Mar;10(3):e305-e306. doi: 10.1016/S2214-109X(21)00572-6. Lancet Glob Health. 2022. PMID: 35180403 Free PMC article. No abstract available.
-
Barriers to statin use in the Philippines.Lancet Glob Health. 2022 Jun;10(6):e796. doi: 10.1016/S2214-109X(22)00201-7. Lancet Glob Health. 2022. PMID: 35561717 No abstract available.
-
Statin use in low-income and middle-income countries.Lancet Glob Health. 2022 Jul;10(7):e954. doi: 10.1016/S2214-109X(22)00219-4. Lancet Glob Health. 2022. PMID: 35714643 No abstract available.
-
Statin use in low-income and middle-income countries - Authors' reply.Lancet Glob Health. 2022 Jul;10(7):e955-e956. doi: 10.1016/S2214-109X(22)00217-0. Lancet Glob Health. 2022. PMID: 35714644 Free PMC article. No abstract available.
References
-
- WHO. Prevention of cardiovascular disease: guidelines for assessment and management of cardiovascular risk. Geneva: World Health Organization, 2007.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
