

INTERGROWTH-21st versus a customized method for the prediction of neonatal nutritional status in hypertensive disorders of pregnancy
- PMID: 35183148
- PMCID: PMC8857827
- DOI: 10.1186/s12884-022-04450-3
INTERGROWTH-21st versus a customized method for the prediction of neonatal nutritional status in hypertensive disorders of pregnancy
Abstract
Background: Hypertensive disorders of pregnancy (HDP) generate complications and are one of the principal causes of maternal, foetal, and neonatal mortality worldwide. It has been observed that in pregnancies with HDP, the incidence of foetuses small for their gestational age (SGA) is twice as high as that in noncomplicated pregnancies. In women with HDP, the identification of foetuses (SGA) is substantially important, as management and follow-up are determined by this information.
Objective: The objective of this study was to evaluate whether the INTERGROWTH-21st method or customized birthweight references better identify newborns with an abnormal nutritional status resulting from HDP.
Method: A comparative analysis study was designed with two diagnostic methods for the prediction of neonatal nutritional status in pregnancies with HDP. The performance of both methods in identifying neonatal malnutrition (defined by a neonatal body mass index < 10th centile or a ponderal index < 10th centile) was assessed by calculating sensitivity, specificity, positive predictive value, negative predictive value, diagnostic odds ratio, Youden's index and probability ratios.
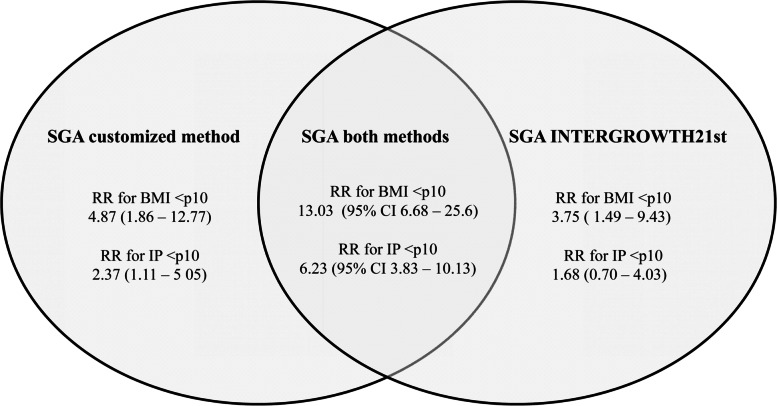
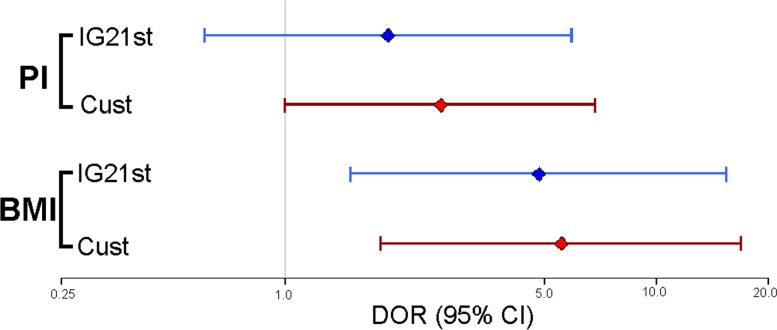
Results: The study included 226 pregnant women diagnosed with HDP. The customized method identified 45 foetuses as small for gestational age (19.9%), while the INTERGROWTH-21st method identified 27 newborns with SGA (11.9%). The difference between proportions was statistically significant (p < 0.01). Using body mass index (< 10th centile) as a measure of nutritional status, newborns identified as SGA by the customized method showed a higher risk of malnutrition than those identified as SGA by INTERGROWTH-21st (RR: 4.87 (95% CI: 1.86-12.77) vs. 3.75 (95% CI: 1.49-9.43)) (DOR: 5.56 (95% CI: 1.82-16.98) vs. 4.84 (95% CI: 1.51-15.54)) Even when using Ponderal index (< 10th centile), newborns identified as SGA by the customized method showed a higher risk of malnutrition than those identified as SGA by INTERGROWTH-21st (RR 2.37 (95% CI: 1.11-5.05) vs. 1.68 (95% CI: 0.70-4.03))(DOR 2.62 (95% CI: 1.00-6.87) vs. 1.90 (95% CI: 0.61-5.92)).
Conclusion: In pregnant women with HDP, the predictive ability of the customized foetal growth curves to identify neonatal malnutrition appears to surpass that of INTERGROWTH-21st.
Keywords: Foetal growth; Foetal malnutrition; Gestational hypertension; Hypertensive disorders of pregnancy; Small for gestational age (SGA).
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
INTERGROWTH-21st vs customized birthweight standards for identification of perinatal mortality and morbidity.Am J Obstet Gynecol. 2016 Apr;214(4):509.e1-509.e7. doi: 10.1016/j.ajog.2015.10.931. Epub 2015 Nov 4. Am J Obstet Gynecol. 2016. PMID: 26546850
-
"INTERGROWTH21st vs customized fetal growth curves in the assessment of the neonatal nutritional status: a retrospective cohort study of gestational diabetes".BMC Pregnancy Childbirth. 2020 Mar 4;20(1):139. doi: 10.1186/s12884-020-2845-y. BMC Pregnancy Childbirth. 2020. PMID: 32131758 Free PMC article.
-
INTERGROWTH-21st compared with GROW customized centiles in the detection of adverse perinatal outcomes at term.J Matern Fetal Neonatal Med. 2020 Mar;33(6):961-966. doi: 10.1080/14767058.2018.1511696. Epub 2018 Oct 29. J Matern Fetal Neonatal Med. 2020. PMID: 30372647
-
Which fetal growth charts should be used? A retrospective observational study in China.Chin Med J (Engl). 2022 Aug 20;135(16):1969-1977. doi: 10.1097/CM9.0000000000002335. Chin Med J (Engl). 2022. PMID: 36070466 Free PMC article. Review.
-
Fetal malnutrition among neonates in African countries: a CAN score systematic review and meta-analysis.Nutr J. 2024 Sep 6;23(1):102. doi: 10.1186/s12937-024-00989-3. Nutr J. 2024. PMID: 39243026 Free PMC article.
Cited by
-
The smaller firstborn: exploring the association of parity and fetal growth.Arch Gynecol Obstet. 2024 Jul;310(1):93-102. doi: 10.1007/s00404-023-07249-5. Epub 2023 Oct 17. Arch Gynecol Obstet. 2024. PMID: 37848678
References
-
- Rochat RW, Koonin LM, Atrash HK, Jewett JF. Maternal mortality in the United States: report from the maternal mortality collaborative. Obstet Gynecol. 1988;72(1):91–97. - PubMed
-
- National High Blood Pressure Education Program Working Group Report on High Blood Pressure in Pregnancy. Am J Obstet Gynecol. 1990;163(5 Pt 1):1691–1712. doi:10.1016/0002-9378(90)90653-o - PubMed
