

TIPS improves outcomes in patients with HCC and symptomatic portal hypertension: a multi-institution experience
- PMID: 35183265
- PMCID: PMC8858571
- DOI: 10.1186/s40644-022-00451-9
TIPS improves outcomes in patients with HCC and symptomatic portal hypertension: a multi-institution experience
Abstract
Background: Hepatocellular carcinoma (HCC) with symptomatic portal hypertension (SPH) has poor prognosis. A transjugular intrahepatic portosystemic shunt (TIPS) relieves SPH, but its application in HCC remains unclear. We evaluated TIPS efficacy in patients with HCC and SPH.
Methods: Pre- and post-TIPS Child-pugh(C-P) scores and stages in 123 HCC patients with SPH from three centers were compared. The impact of postoperative C-P stage indicators on overall survival (OS) was explored.
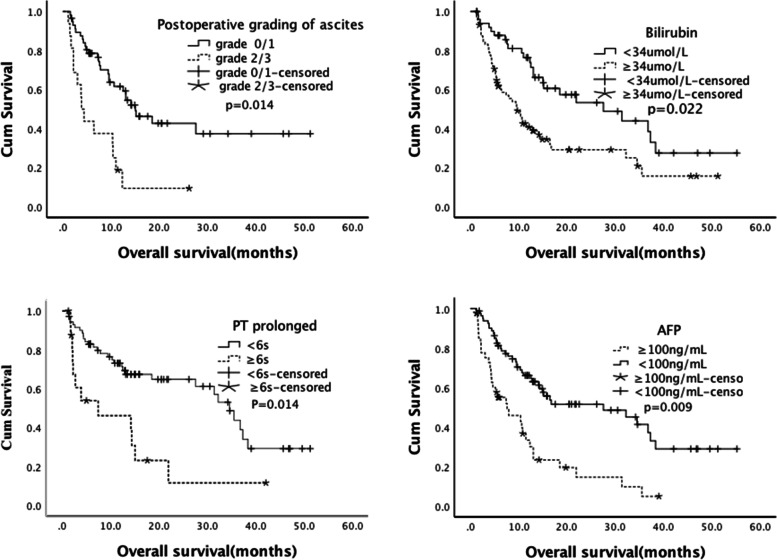
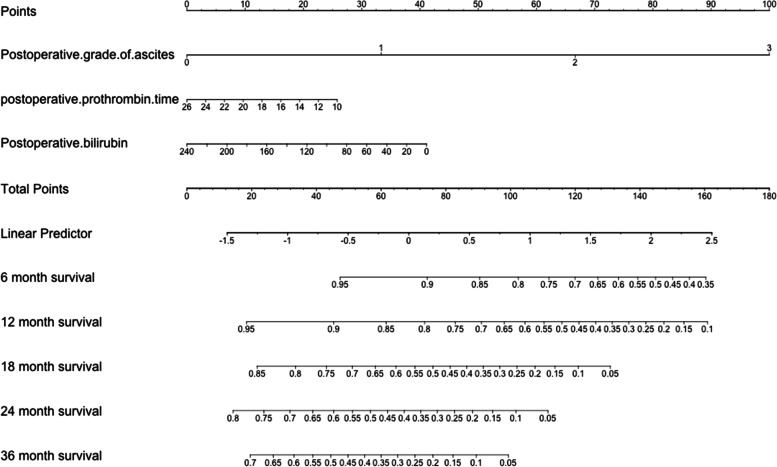
Results: Post-TIPS responses to SPH included complete response (CR) (92 [74.8%]), partial response (PR) (23 [18.7%]), and nonresponse (NR) (8 [6.5%]). The control (proportion of CR and PR) for SPH was 93.5%. Median C-P scores pre-TIPS and at one month post-TIPS were 8 (IQR 6-9) and 7 (IQR 6-8), respectively (P < 0.001). Forty-one (33.3%) patients had C-P downstaging; 73 (59.3%) had lowered C-P scores; and 73 (59.3%) received intrahepatic local therapy post-TIPS. The median OS was 10.7 (1.1-55.2) months. Among the five indicators of C-P stage, lower post-TIPS ascites grading [(0/1)/(2/3); P = 0.014, HR = 0.31 (95% CI: 0.12-0.79)] and bilirubin [< 34/ ≥ 34 µmol/L; P = 0.022, HR = 0.47 (95% CI: 0.23-0.82)] and prothrombin time prolongation < 6 s [< 6/ ≥ 6 s; P = 0.001, HR = 0.17 (95% CI: 0.06-0.47)] were independent protective indicators of OS. These three indicators were included in the nomogram model to predict survival probabilities.
Conclusions: TIPS is safe and effective for HCC with SPH. This procedure can relieve the symptoms, enable subsequent antitumor therapy, and bring survival benefits, possibly through improved liver function by reducing C-P stage.
Keywords: Child–Pugh stage; Hepatocellular carcinoma; Portal hypertension; TIPS.
© 2022. The Author(s).
Conflict of interest statement
We declare no competing interests.
Figures
Similar articles
-
The Role of Transjugular Intrahepatic Portosystemic Shunt (TIPS) in Treating Portal Hypertension in Patients with Hepatocellular Carcinoma.Medicina (Kaunas). 2023 Jun 15;59(6):1150. doi: 10.3390/medicina59061150. Medicina (Kaunas). 2023. PMID: 37374354 Free PMC article. Review.
-
TIPS plus sequential systemic therapy of advanced HCC patients with tumour thrombus-related symptomatic portal hypertension.Eur Radiol. 2022 Oct;32(10):6777-6787. doi: 10.1007/s00330-022-08705-7. Epub 2022 Apr 20. Eur Radiol. 2022. PMID: 35441840 Free PMC article.
-
Combined transjugular intrahepatic portosystemic shunt and other interventions for hepatocellular carcinoma with portal hypertension.World J Gastroenterol. 2015 Nov 21;21(43):12439-47. doi: 10.3748/wjg.v21.i43.12439. World J Gastroenterol. 2015. PMID: 26604651 Free PMC article.
-
Investigating the risk factors of hepatocellular carcinoma and survival analysis for cirrhosis after transjugular intrahepatic portosystemic shunt in treating portal hypertension.J Cancer Res Ther. 2018;14(4):826-832. doi: 10.4103/jcrt.JCRT_930_17. J Cancer Res Ther. 2018. PMID: 29970660
-
Transjugular intrahepatic portosystemic shunts and portal hypertension-related complications.World J Gastroenterol. 2014 Dec 7;20(45):16996-7010. doi: 10.3748/wjg.v20.i45.16996. World J Gastroenterol. 2014. PMID: 25493012 Free PMC article. Review.
Cited by
-
Risks and benefits of TIPS in HCC and other liver malignancies: a literature review.BMC Gastroenterol. 2023 Nov 20;23(1):403. doi: 10.1186/s12876-023-03047-0. BMC Gastroenterol. 2023. PMID: 37986043 Free PMC article. Review.
-
Efficacy and safety of TACE combined with TKIs and PD-1 inhibitors in HCC patients with prior TIPS.Front Oncol. 2025 Apr 24;15:1570029. doi: 10.3389/fonc.2025.1570029. eCollection 2025. Front Oncol. 2025. PMID: 40342829 Free PMC article.
-
Efficacy and safety of transjugular intrahepatic portosystemic shunt in patients with hepatocellular carcinoma-A systematic review and meta-analysis.Indian J Gastroenterol. 2024 Dec;43(6):1121-1135. doi: 10.1007/s12664-024-01646-7. Epub 2024 Aug 10. Indian J Gastroenterol. 2024. PMID: 39126599
-
Transjugular Intrahepatic Portosystemic Shunt for Advanced Hepatocellular Carcinoma With Main Portal Vein Tumor Thrombus-Related Symptomatic Portal Hypertension.J Clin Exp Hepatol. 2024 Mar-Apr;14(2):101305. doi: 10.1016/j.jceh.2023.101305. Epub 2023 Nov 18. J Clin Exp Hepatol. 2024. PMID: 38130294 Free PMC article.
-
The Role of Transjugular Intrahepatic Portosystemic Shunt (TIPS) in Treating Portal Hypertension in Patients with Hepatocellular Carcinoma.Medicina (Kaunas). 2023 Jun 15;59(6):1150. doi: 10.3390/medicina59061150. Medicina (Kaunas). 2023. PMID: 37374354 Free PMC article. Review.
References
-
- Bray F, Ferlay J, Soerjomataram I. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians; 2018. - PubMed
-
- Angeli P , Bernardi M , Villanueva, Càndid, et al. European Association for the Study of the Liver, EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69:406–60. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
