

Abnormal dynamic ventilation function of COVID-19 survivors detected by pulmonary free-breathing proton MRI
- PMID: 35184219
- PMCID: PMC8858033
- DOI: 10.1007/s00330-022-08605-w
Abnormal dynamic ventilation function of COVID-19 survivors detected by pulmonary free-breathing proton MRI
Abstract
Objectives: To visualize and quantitatively assess regional lung function of survivors of COVID-19 who were hospitalized using pulmonary free-breathing 1H MRI.
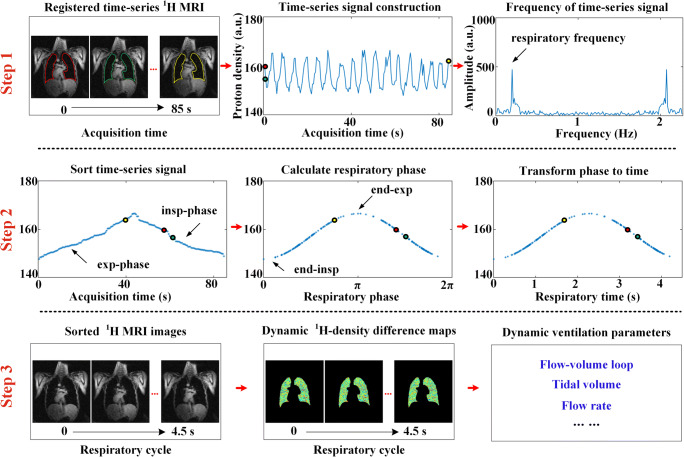
Methods: A total of 12 healthy volunteers and 27 COVID-19 survivors (62.4 ± 8.1 days between infection and image acquisition) were recruited in this prospective study and performed chest 1H MRI acquisitions with free tidal breathing. Then, conventional Fourier decomposition ventilation (FD-V) and global fractional ventilation (FVGlobal) were analyzed. Besides, a modified PREFUL (mPREFUL) method was developed to adapt to COVID-19 survivors and generate dynamic ventilation maps and parameters. All the ventilation maps and parameters were analyzed using Student's t-test. Pearson's correlation and a Bland-Altman plot between FVGlobal and mPREFUL were analyzed.
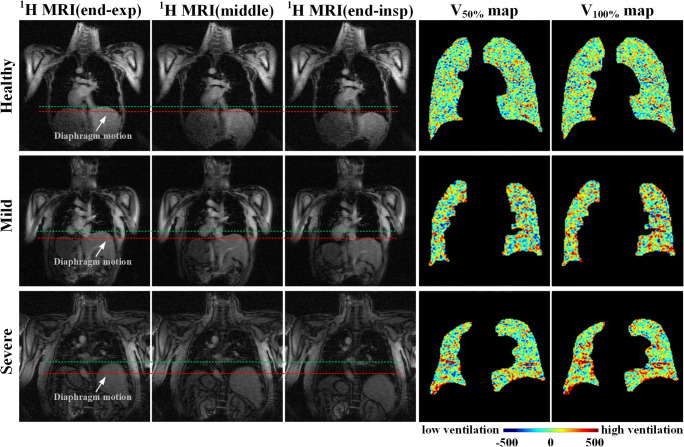
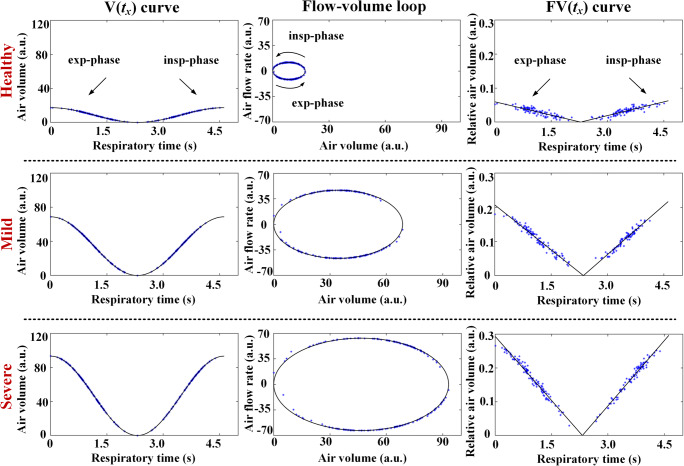
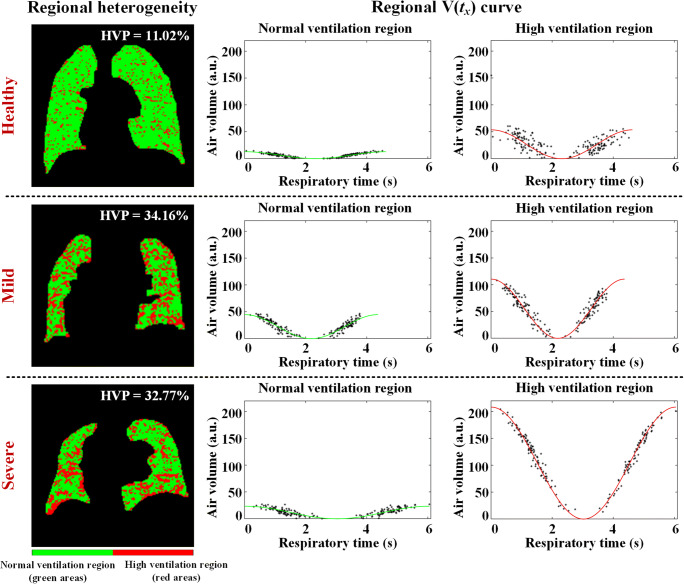
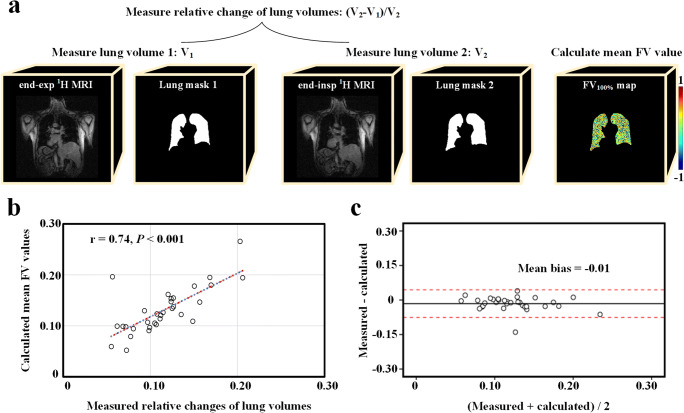
Results: There was no significant difference between COVID-19 and healthy groups regarding a static FD-V map (0.47 ± 0.12 vs 0.42 ± 0.08; p = .233). However, mPREFUL demonstrated lots of regional high ventilation areas (high ventilation percentage (HVP): 23.7% ± 10.6%) existed in survivors. This regional heterogeneity (i.e., HVP) in survivors was significantly higher than in healthy volunteers (p = .003). The survivors breathed deeper (flow-volume loop: 5375 ± 3978 vs 1688 ± 789; p = .005), and breathed more air in respiratory cycle (total amount: 62.6 ± 19.3 vs 37.3 ± 9.9; p < .001). Besides, mPREFUL showed both good Pearson's correlation (r = 0.74; p < .001) and Bland-Altman consistency (mean bias = -0.01) with FVGlobal.
Conclusions: Dynamic ventilation imaging using pulmonary free-breathing 1H MRI found regional abnormity of dynamic ventilation function in COVID-19 survivors.
Key points: • Pulmonary free-breathing1H MRI was used to visualize and quantitatively assess regional lung ventilation function of COVID-19 survivors. • Dynamic ventilation maps generated from 1H MRI were more sensitive to distinguish the COVID-19 and healthy groups (total air amount: 62.6 ± 19.3 vs 37.3 ± 9.9; p < .001), compared with static ventilation maps (FD-V value: 0.47 ± 0.12 vs 0.42 ± 0.08; p = .233). • COVID-19 survivors had larger regional heterogeneity (high ventilation percentage: 23.7% ± 10.6% vs 13.1% ± 7.9%; p = .003), and breathed deeper (flow-volume loop: 5375 ± 3978 vs 1688 ± 789; p = .005) than healthy volunteers.
Keywords: COVID-19 survivors; Dynamic ventilation imaging; Phase-resolved functional lung (PREFUL); Pulmonary free-breathing 1H MRI; Regional lung function.
© 2022. The Author(s), under exclusive licence to European Society of Radiology.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- World Health Organization (2021) Coronavirus disease (COVID-2019) situation reports. Available via https://www.who.int/publications/m/item/weekly-operational-update-on-cov.... Accessed 2 Dec 2021
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
