

Timing of antimicrobial prophylaxis for cesarean section is critical for gut microbiome development in term born infants
- PMID: 35184691
- PMCID: PMC8865290
- DOI: 10.1080/19490976.2022.2038855
Timing of antimicrobial prophylaxis for cesarean section is critical for gut microbiome development in term born infants
Abstract
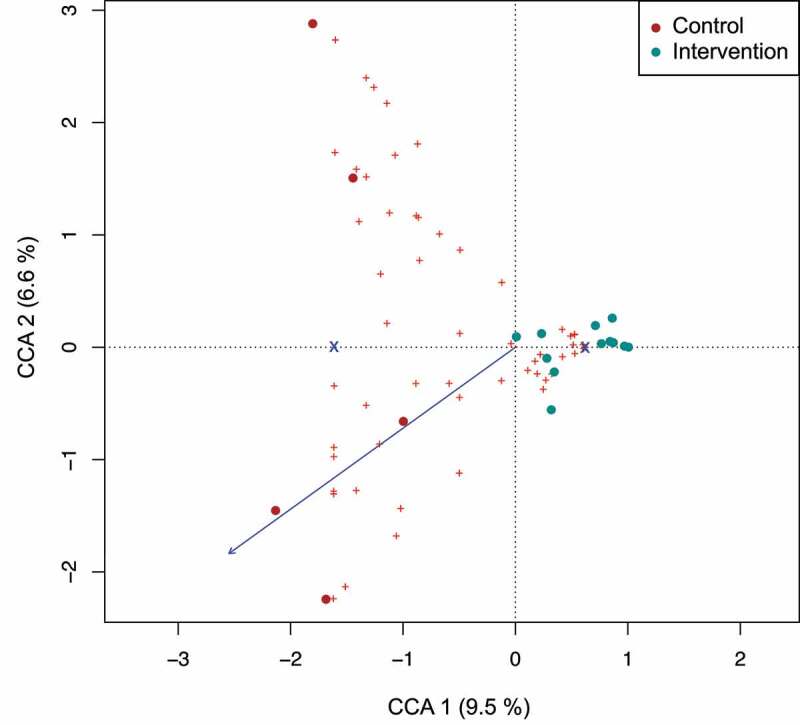
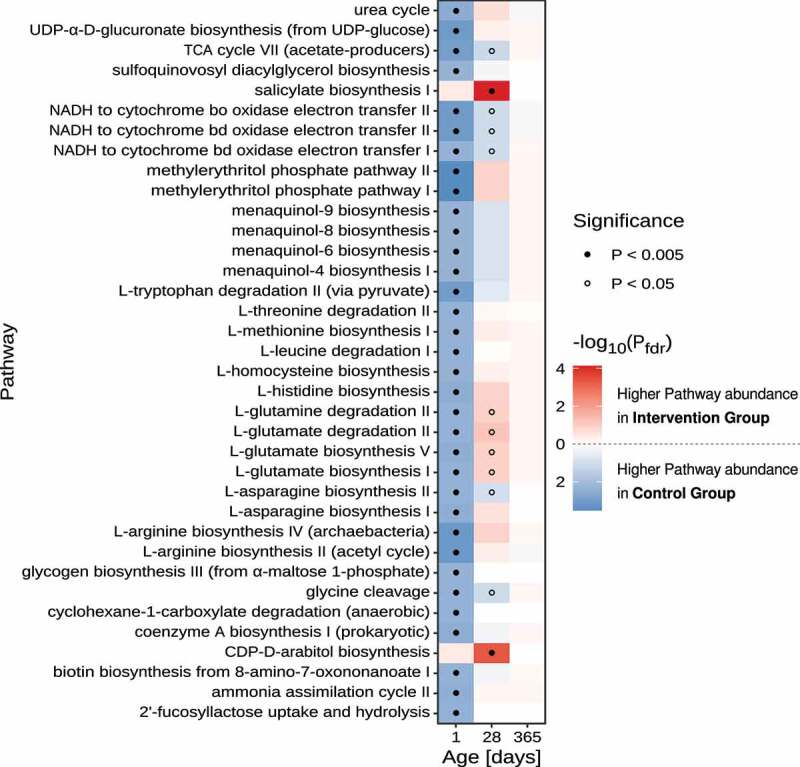
Animal models imply that the perinatal exposure to antibiotics has a substantial impact on microbiome establishment of the offspring. We aimed to evaluate the effect of timing of antimicrobial prophylaxis for cesarean section before versus after cord clamping on gut microbiome composition of term born infants. We performed an exploratory, single center randomized controlled clinical trial. We included forty pregnant women with elective cesarean section at term. The intervention group received single dose intravenous cefuroxime after cord clamping (n = 19), the control group single dose intravenous cefuroxime 30 minutes before skin incision (n = 21). The primary endpoint was microbiome signature of infants and metabolic prediction in the first days of life as determined in meconium samples by 16S rRNA gene sequencing. Secondary endpoints were microbiome composition at one month and 1 year of life. In meconium samples of the intervention group, the genus Staphylococcus pre-dominated. In the control group, the placental cross-over of cefuroxime was confirmed in cord blood. A higher amino acid and nitrogen metabolism as well as increased abundance of the genera Cutibacterium, Corynebacterium and Streptophyta were noted (indicator families: Cytophagaceae, Lactobacilaceae, Oxalobacteraceae). Predictive models of metabolic function revealed higher 2'fucosyllactose utilization in control group samples. In the follow-up visits, a higher abundance of the genus Clostridium was evident in the intervention group. Our exploratory randomized controlled trial suggests that timing of antimicrobial prophylaxis is critical for early microbiome engraftment but not antimicrobial resistance emergence in term born infants.
Keywords: Microbiome; antibiotic resistome; antibiotics; cesarean section; diversity; surgical antimicrobial prophylaxis; term infant.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures




References
-
- Institut für Qualitätssicherung und Transparenz im Gesundheitswesen . Bundesauswertung zum Erfassungsjahr 2019 Geburtshilfe. 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources