

T2/FLAIR Abnormity Could be the Sign of Glioblastoma Dissemination
- PMID: 35185770
- PMCID: PMC8849106
- DOI: 10.3389/fneur.2022.819216
T2/FLAIR Abnormity Could be the Sign of Glioblastoma Dissemination
Abstract
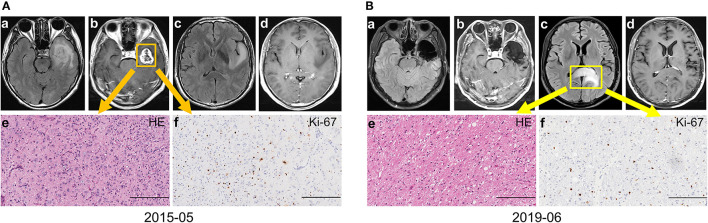
Purpose: Newly emerged or constantly enlarged contrast-enhancing (CE) lesions were the necessary signs for the diagnosis of glioblastoma (GBM) progression. This study aimed to investigate whether the T2-weighted-Fluid-Attenuated Inversion Recovery (T2/FLAIR) abnormal transformation could predict and assess progression for GBMs, especially for tumor dissemination.
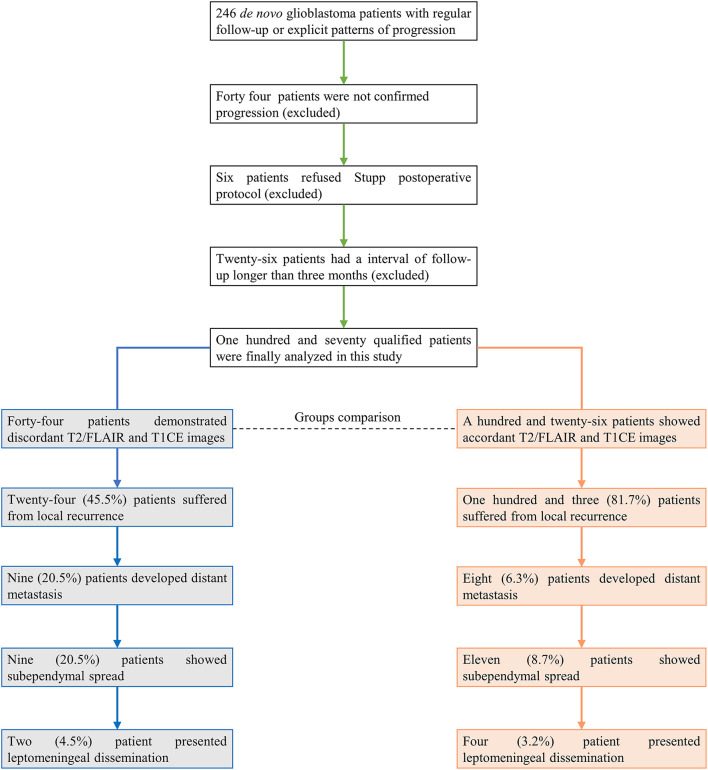
Methods: A consecutive cohort of 246 GBM patients with regular follow-up and sufficient radiological data was included in this study. The series of T2/FLAIR and T1CE images were retrospectively reviewed. The patients were separated into T2/FLAIR and T1CE discordant and accordant subgroups based on the initial progression images.
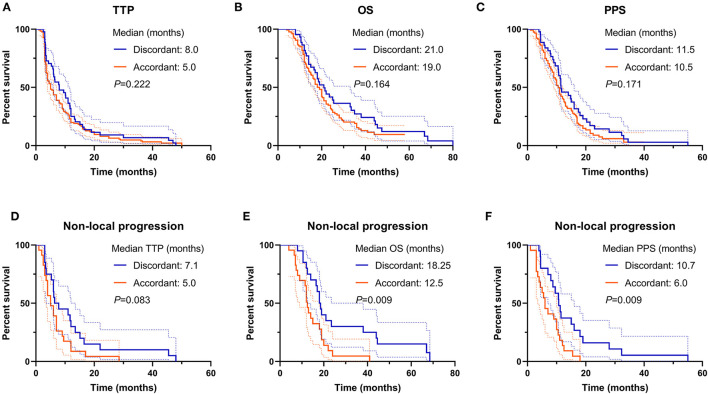
Results: A total of 170 qualified patients were finally analyzed. The incidence of discordant T2/FLAIR and T1CE images was 25.9% (44/170). The median time-span of T2/FLAIR indicated tumor progression was 119.5 days (ranging from 57 days-unreached) prior to T1CE. Nearly half of patients (20/44, 45.5%) in the discordant subgroup suffered from tumor dissemination, substantially higher than accordant patients (23/126, 20.6%, p < 0.001). The median time to progression (TTP), post-progression survival (PPS), and overall survival (OS) were not statistically different (all p > 0.05) between discordant and accordant patients.
Conclusions: T2/FLAIR abnormity could be the sign of GBM progression, especially for newly emerged lesions disseminating from the primary cavity. Physicians should cast more attention on the dynamic change of T2/FLAIR images, which might be of great significance for progression assessment and subsequent clinical decision-making.
Keywords: RANO; T2/FLAIR; dissemination; glioblastoma (GBM); gross total removal of tumor (GTR); isocitrate dehydrogenase (IDH); progression; supratotal maximal resection (SMR).
Copyright © 2022 Li, Huang, Chen, Jiang, Yang, Shen, Cui, Dong, Ren and Lin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Subventricular zone-associated classification in isocitrate dehydrogenase-wildtype glioblastomas: improved prognostic value through integration of FLAIR with contrast-enhanced imaging.J Neurosurg. 2024 Jun 28;141(5):1304-1313. doi: 10.3171/2024.4.JNS232658. Print 2024 Nov 1. J Neurosurg. 2024. PMID: 38941641
-
T2 Fluid-Attenuated Inversion Recovery Resection for Glioblastoma Involving Eloquent Brain Areas Facilitated Through Awake Craniotomy and Clinical Outcome.World Neurosurg. 2020 Mar;135:e738-e747. doi: 10.1016/j.wneu.2019.12.130. Epub 2019 Dec 30. World Neurosurg. 2020. PMID: 31899397
-
Extending the resection beyond the contrast-enhancement for glioblastoma: feasibility, efficacy, and outcomes.Br J Neurosurg. 2018 Oct;32(5):528-535. doi: 10.1080/02688697.2018.1498450. Epub 2018 Aug 3. Br J Neurosurg. 2018. PMID: 30073866
-
A systematic review and meta-analysis of supratotal versus gross total resection for glioblastoma.J Neurooncol. 2020 Jul;148(3):419-431. doi: 10.1007/s11060-020-03556-y. Epub 2020 Jun 19. J Neurooncol. 2020. PMID: 32562247
-
The T2-FLAIR-mismatch sign as an imaging biomarker for IDH and 1p/19q status in diffuse low-grade gliomas: a systematic review with a Bayesian approach to evaluation of diagnostic test performance.Neurosurg Focus. 2019 Dec 1;47(6):E13. doi: 10.3171/2019.9.FOCUS19660. Neurosurg Focus. 2019. PMID: 31786548
Cited by
-
Supramaximal versus gross total resection in Glioblastoma, IDH wild-type and Astrocytoma, IDH-mutant, grade 4, effect on overall and progression free survival: systematic review and meta-analysis.J Neurooncol. 2023 Aug;164(1):31-41. doi: 10.1007/s11060-023-04409-0. Epub 2023 Aug 10. J Neurooncol. 2023. PMID: 37561356
-
Biological underpinnings of radiomic magnetic resonance imaging phenotypes for risk stratification in IDH wild-type glioblastoma.J Transl Med. 2023 Nov 22;21(1):841. doi: 10.1186/s12967-023-04551-3. J Transl Med. 2023. PMID: 37993907 Free PMC article.
-
Prognostic factors affecting outcome of multifocal or multicentric glioblastoma: A scoping review.J Neurosci Rural Pract. 2023 Apr-Jun;14(2):199-209. doi: 10.25259/JNRP_41_2022. Epub 2022 Dec 15. J Neurosci Rural Pract. 2023. PMID: 37181186 Free PMC article.
-
The Three Pillars of Glioblastoma: A Systematic Review and Novel Analysis of Multi-Omics and Clinical Data.Cells. 2024 Oct 23;13(21):1754. doi: 10.3390/cells13211754. Cells. 2024. PMID: 39513861 Free PMC article.
-
Histologic Definition of Enhancing Core and FLAIR Hyperintensity Region of Glioblastoma, IDH-Wild Type: A Clinico-Pathologic Study on a Single-Institution Series.Brain Sci. 2023 Jan 31;13(2):248. doi: 10.3390/brainsci13020248. Brain Sci. 2023. PMID: 36831791 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous