

Effectiveness of ustekinumab in patients with refractory Crohn's disease: a multicentre real-life study in Italy
- PMID: 35186121
- PMCID: PMC8848093
- DOI: 10.1177/17562848211072412
Effectiveness of ustekinumab in patients with refractory Crohn's disease: a multicentre real-life study in Italy
Abstract
Background: The effectiveness of ustekinumab in patients with refractory Crohn's disease (CD) has been investigated in several real-world studies. However, very few data concerning the real-life experience in Italy have been reported. Therefore, this study assessed the effectiveness of ustekinumab in a large cohort of Italian patients with refractory CD.
Methods: All patients who had started on ustekinumab after failure of or intolerance to antitumour necrosis factor-α (TNF-α) treatment at five tertiary centres between November 2018 and February 2020 were retrospectively enrolled. The coprimary outcome was corticosteroid-free clinical remission, defined as a Harvey-Bradshaw Index (HBI) score of ⩽4, at weeks 26 and 52. The secondary outcomes were changes in the HBI and C-reactive protein (CRP) values at weeks 8, 26, and 52 from baseline and the normalization of CRP in patients with initially abnormal values.
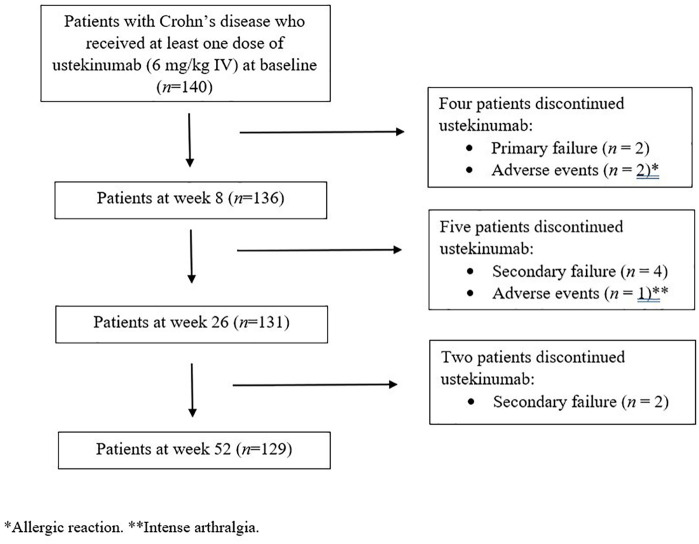
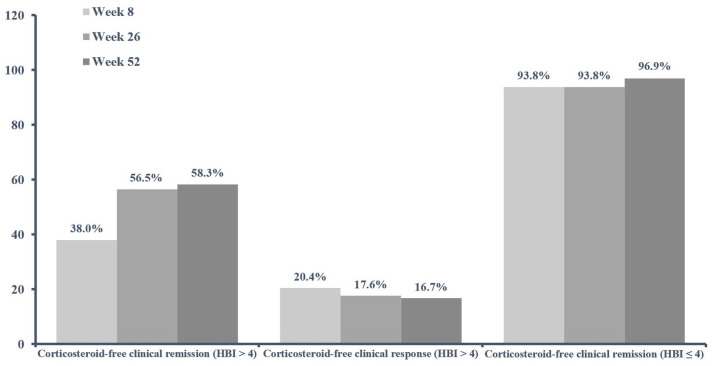
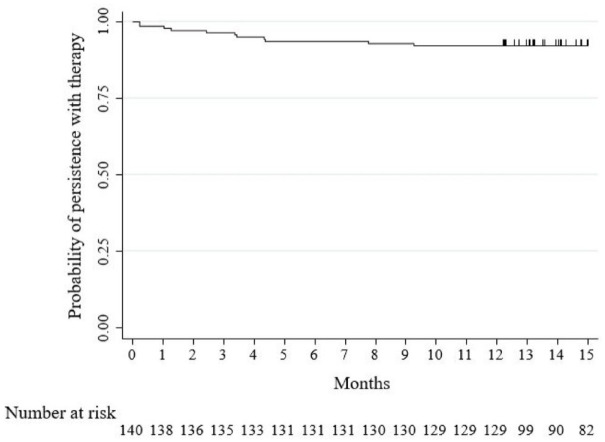
Results: Totally, 140 patients who had previously received at least one anti-TNF-α agent were enrolled; 40.0% received two anti-TNF-α agents and 20.0% received vedolizumab. At baseline, 108 patients (77.1%) had HBI scores of >4; of these, 56.5% and 58.3% achieved corticosteroid-free clinical remission at weeks 26 and 52, respectively. Significant decreases in HBI and CRP values were observed at weeks 8, 26, and 52 in the entire study cohort (all p < 0.0001). The CRP values were normalized in 34.9%, 37.8%, and 49.3% of the patients by weeks 8, 26, and 52, respectively. The baseline HBI score of ⩾8 was a negative predictor of corticosteroid-free clinical remission at week 52 (odds ratio: 0.21, 95% confidence interval: 0.08-0.56, p = 0.002). The probability of remaining on ustekinumab after 52 weeks was 92.1%. Eleven (7.9%) patients discontinued ustekinumab (three for adverse events).
Conclusion: Our study findings confirm the effectiveness and safety of ustekinumab in patients with CD after failure of or intolerance to anti-TNF-α therapy.
Keywords: Crohn’s disease; effectiveness; refractory; ustekinumab.
© The Author(s), 2022.
Conflict of interest statement
Conflict of interest statement: The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MLS: advisory board and/or lecture fees from AbbVie, Celltrion, Janssen, Pfizer, and Takeda. CB: lecture fees from Takeda, AbbVie, and Janssen. SS: advisory board and lecture fees from Arena, Gilead, Janssen, Takeda, and AbbVie. CP: consultancy fees and/or educational grants from AbbVie, MSD, Takeda, Pfizer, Janssen-Cilag, Chiesi, Sofar, Ferring, and Zambon. LB: speaker fees from Ferring, AbbVie, Janssen, and Zambon. The other authors declare no conflict of interest.
Figures
References
-
- Torres J, Mehandru S, Colombel JF, et al.. Crohn’s disease. Lancet 2017; 389: 1741–1755. - PubMed
-
- Orlando A, Armuzzi A, Papi C, et al.. The Italian Society of Gastroenterology (SIGE) and the Italian Group for the study of Inflammatory Bowel Disease (IG-IBD) clinical practice guidelines: the use of tumor necrosis factor-alpha antagonist therapy in inflammatory bowel disease. Dig Liver Dis 2011; 43: 1–20. - PubMed
-
- Nielsen OH, Ainsworth MA. Tumor necrosis factor inhibitors for inflammatory bowel disease. N Engl J Med 2013; 369: 754–762. - PubMed
-
- Ding NS, Hart A, De Cruz P. Systematic review: predicting and optimising response to anti-TNF therapy in Crohn’s disease – algorithm for practical management. Aliment Pharmacol Ther 2016; 43: 30–51. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
