Machine learning models compared to existing criteria for noninvasive prediction of endoscopic retrograde cholangiopancreatography-confirmed choledocholithiasis
- PMID: 35186364
- PMCID: PMC8855981
- DOI: 10.1016/j.livres.2021.10.001
Machine learning models compared to existing criteria for noninvasive prediction of endoscopic retrograde cholangiopancreatography-confirmed choledocholithiasis
Abstract
Background and aims: Noninvasive predictors of choledocholithiasis have generally exhibited marginal performance characteristics. We aimed to identify noninvasive independent predictors of endoscopic retrograde cholangiopancreatography (ERCP)-confirmed choledocholithiasis and accordingly developed predictive machine learning models (MLMs).
Methods: Clinical data of consecutive patients undergoing first-ever ERCP for suspected choledocholithiasis from 2015-2019 were abstracted from a prospectively-maintained database. Multiple logistic regression was used to identify predictors of ERCP-confirmed choledocholithiasis. MLMs were then trained to predict ERCP-confirmed choledocholithiasis using pre-ERCP ultrasound (US) imaging only and separately using all available noninvasive imaging (US/CT/magnetic resonance cholangiopancreatography). The diagnostic performance of American Society for Gastrointestinal Endoscopy (ASGE) "high-likelihood" criteria was compared to MLMs.
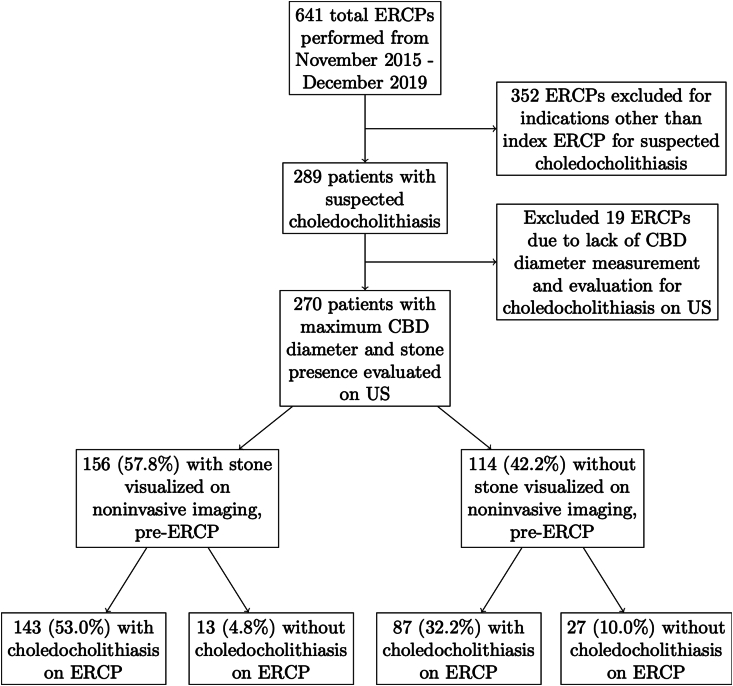
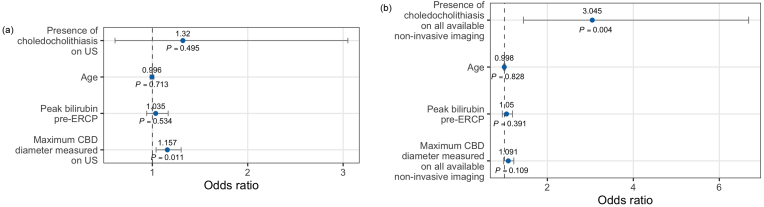
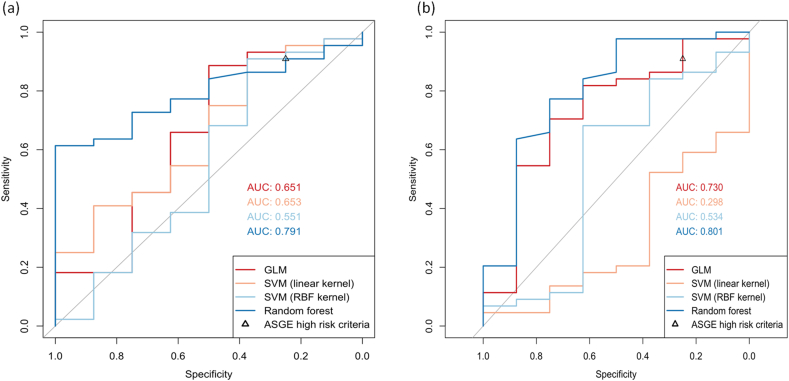
Results: We identified 270 patients (mean age 46 years, 62.2% female, 73.7% Hispanic/Latino, 59% with noninvasive imaging positive for choledocholithiasis) with native papilla who underwent ERCP for suspected choledocholithiasis, of whom 230 (85.2%) were found to have ERCP-confirmed choledocholithiasis. Logistic regression identified choledocholithiasis on noninvasive imaging (odds ratio (OR) = 3.045, P = 0.004) and common bile duct (CBD) diameter on noninvasive imaging (OR=1.157, P = 0.011) as predictors of ERCP-confirmed choledocholithiasis. Among the various MLMs trained, the random forest-based MLM performed best; sensitivity was 61.4% and 77.3% and specificity was 100% and 75.0%, using US-only and using all available imaging, respectively. ASGE high-likelihood criteria demonstrated sensitivity of 90.9% and specificity of 25.0%; using cut-points achieving this specificity, MLMs achieved sensitivity up to 97.7%.
Conclusions: MLMs using age, sex, race, presence of diabetes, fever, body mass index (BMI), total bilirubin, maximum CBD diameter, and choledocholithiasis on pre-ERCP noninvasive imaging predict ERCP-confirmed choledocholithiasis with good sensitivity and specificity and outperform the ASGE criteria for patients with suspected choledocholithiasis.
Keywords: Bile duct disorders; Common bile duct stones; Endoscopic retrograde cholangiopancreatography (ERCP); Gallstones; Machine learning models (MLMs); Noninvasive imaging.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no conflict of interest.
Figures