

External validation of five predictive models for postoperative cardiopulmonary morbidity in a Chinese population receiving lung resection
- PMID: 35186502
- PMCID: PMC8840067
- DOI: 10.7717/peerj.12936
External validation of five predictive models for postoperative cardiopulmonary morbidity in a Chinese population receiving lung resection
Abstract
Background: No postoperative cardiopulmonary morbidity models have been developed or validated in Chinese patients with lung resection. This study aims to externally validate five predictive models, including Eurolung models, the Brunelli model and the Age-adjusted Charlson Comorbidity Index, in a Chinese population.
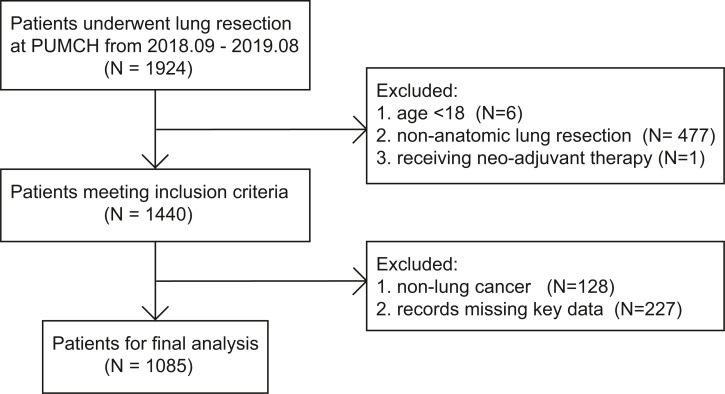
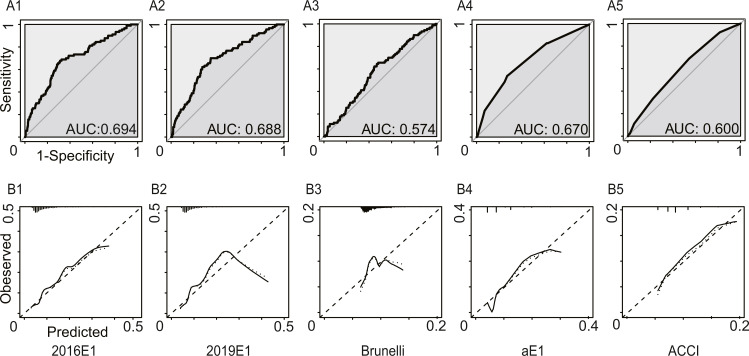
Methods: Patients with lung cancer who underwent anatomic lung resection between 2018/09/01 and 2019/08/31 in our center were involved. Model discrimination was assessed by the area under the receiver operating characteristic curve. Model calibration was evaluated by the Hosmer-Lemeshow test. Calibration curves were plotted. Specificity, sensitivity, negative predictive value, positive predictive value and accuracy were calculated. Model updating was achieved by re-estimating the intercept and/or the slope of the linear predictor and re-estimating all coefficients.
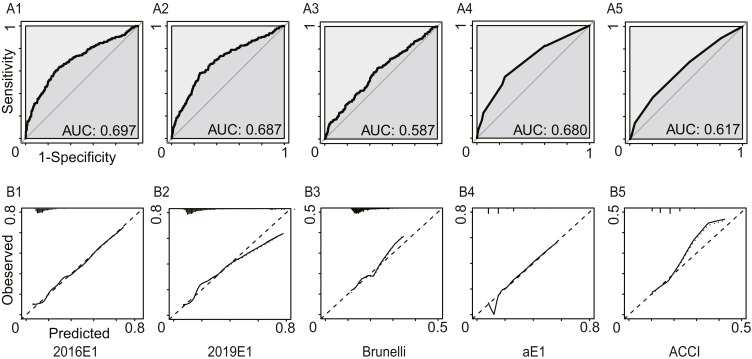
Results: Among 1085 patients, 91 patients had postoperative cardiopulmonary complications defined by the European Society of Thoracic Surgeons. For original models, only parsimonious Eurolung1 had acceptable discrimination (area under the receiver operating characteristic curve = 0.688, 95% confidence interval 0.630-0.745) and calibration (p = 0.23 > 0.05) abilities simultaneously. Its sensitivity, specificity, positive predictive value, negative predictive value and accuracy were 0.700, 0.649, 0.153, 0.960 and 0.653, respectively. In the secondary analysis, increased pleural effusion (n = 94), which was nonchylous and nonpurulent, was labeled as a kind of postoperative complication. The area under the receiver operating characteristic curve of the models increased slightly, but all models were miscalibrated. The original Eurolung1 model had the highest discrimination ability but poor calibration, and thus it was updated by three methods. After model updating, new models showed good calibration and small improvements in discrimination. The discrimination ability was still merely acceptable.
Conclusions: Overall, none of the models performed well on postoperative cardiopulmonary morbidity prediction in this Chinese population. The original parsimonious Eurolung1 and the updated Eurolung1 were the best-performing models on morbidity prediction, but their discrimination ability only achieved an acceptable level. A multicenter study with more relevant variables and sophisticated statistical methods is warranted to develop new models among Chinese patients in the future.
Keywords: Lung cancer; Morbidity; Predictive models; Validation.
©2022 Huang et al.
Conflict of interest statement
The authors declare there are no competing interests.
Figures
Similar articles
-
External validation of the European Society of Thoracic Surgeons morbidity and mortality risk models.Eur J Cardiothorac Surg. 2022 Aug 3;62(3):ezac170. doi: 10.1093/ejcts/ezac170. Eur J Cardiothorac Surg. 2022. PMID: 35301527
-
Parsimonious Eurolung risk models to predict cardiopulmonary morbidity and mortality following anatomic lung resections: an updated analysis from the European Society of Thoracic Surgeons database.Eur J Cardiothorac Surg. 2020 Mar 1;57(3):455-461. doi: 10.1093/ejcts/ezz272. Eur J Cardiothorac Surg. 2020. PMID: 31605105
-
External validation of risk prediction scores in patients undergoing anatomic video-assisted thoracoscopic resection.Surg Endosc. 2023 Apr;37(4):2789-2799. doi: 10.1007/s00464-022-09786-7. Epub 2022 Dec 7. Surg Endosc. 2023. PMID: 36477642 Free PMC article.
-
A discussion of calibration techniques for evaluating binary and categorical predictive models.Prev Vet Med. 2018 Jan 1;149:107-114. doi: 10.1016/j.prevetmed.2017.11.018. Epub 2017 Nov 24. Prev Vet Med. 2018. PMID: 29290291 Review.
-
Risk prediction models for incident type 2 diabetes in Chinese people with intermediate hyperglycemia: a systematic literature review and external validation study.Cardiovasc Diabetol. 2022 Sep 13;21(1):182. doi: 10.1186/s12933-022-01622-5. Cardiovasc Diabetol. 2022. PMID: 36100925 Free PMC article.
Cited by
-
Interpretable prediction of cardiopulmonary complications after non-small cell lung cancer surgery based on machine learning and SHapley additive exPlanations.Heliyon. 2023 Jul 3;9(7):e17772. doi: 10.1016/j.heliyon.2023.e17772. eCollection 2023 Jul. Heliyon. 2023. PMID: 37483738 Free PMC article.
-
Prediction of postoperative cardiopulmonary complications after lung resection in a Chinese population: A machine learning-based study.Front Oncol. 2022 Sep 23;12:1003722. doi: 10.3389/fonc.2022.1003722. eCollection 2022. Front Oncol. 2022. PMID: 36212485 Free PMC article.
-
Impact of surgical approach on 90-day mortality after lung resection for nonsmall cell lung cancer in high-risk operable patients.ERJ Open Res. 2024 Jan 22;10(1):00653-2023. doi: 10.1183/23120541.00653-2023. eCollection 2024 Jan. ERJ Open Res. 2024. PMID: 38259816 Free PMC article.
References
-
- Bendixen M, Jørgensen OD, Kronborg C, Andersen C, Licht PB. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. The Lancet Oncology. 2016;17:836–844. doi: 10.1016/s1470-2045(16)00173-x. - DOI - PubMed
-
- Benker M, Citak N, Neuer T, Opitz I, Inci I. Impact of preoperative comorbidities on postoperative complication rate and outcome in surgically resected non-small cell lung cancer patients. General Thoracic and Cardiovascular Surgery. 2021 doi: 10.1007/s11748-021-01710-5. Epub ahead of print Sep 23 2021. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
