

Efficacy of Quadratus Lumborum Block for Pain Control in Patients Undergoing Hip Surgeries: A Systematic Review and Meta-Analysis
- PMID: 35186969
- PMCID: PMC8850973
- DOI: 10.3389/fmed.2021.771859
Efficacy of Quadratus Lumborum Block for Pain Control in Patients Undergoing Hip Surgeries: A Systematic Review and Meta-Analysis
Abstract
Background: Several studies have reported the use of anterior, posterior and lateral quadratus lumborum block (QLB) for pain control in hip surgeries. However, high-quality evidence is lacking. The current review aimed to summarize data on the efficacy of QLB for pain control in patients undergoing hip surgeries.
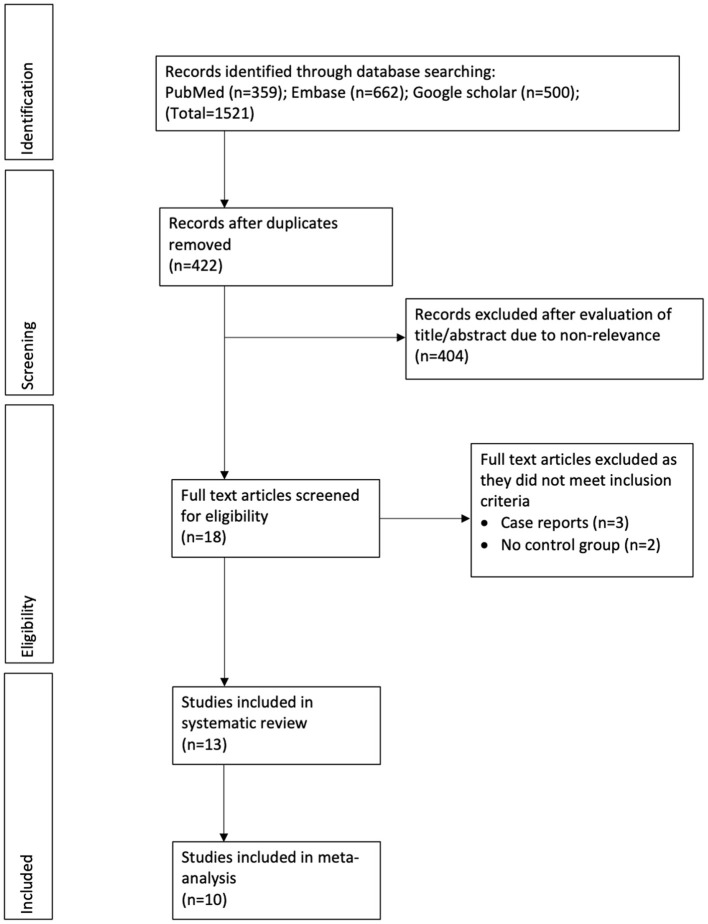
Methods: PubMed, Embase, and Google Scholar databases were searched up to August 5, 2021 for randomized controlled trials (RCTs) or non-RCTs assessing the efficacy of QLB for any type of hip surgery.
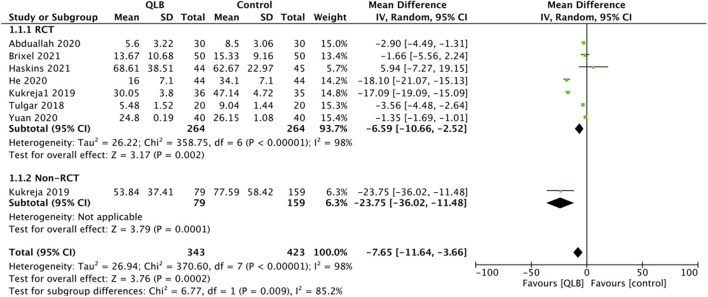
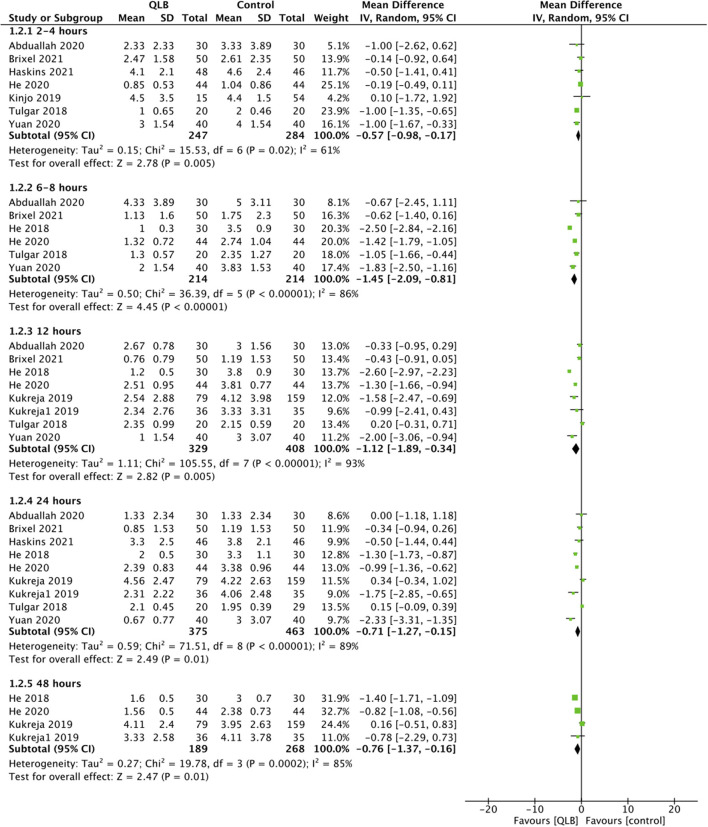
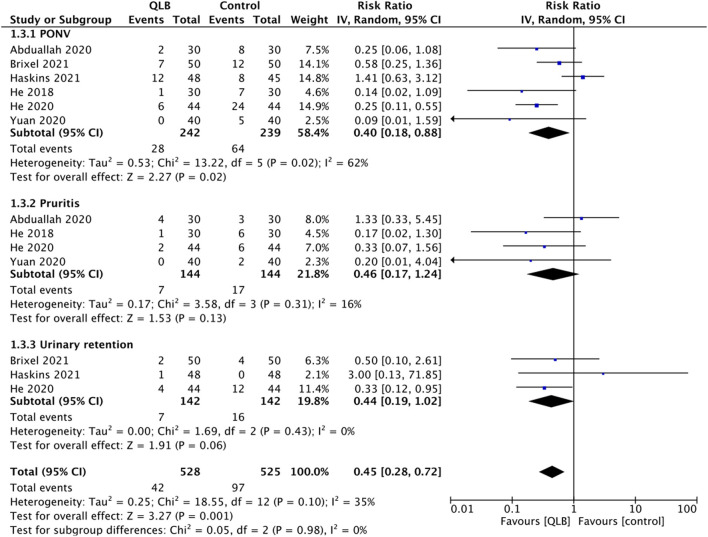
Results: Thirteen studies were included (nine RCTs and four non-RCTs). On pooled analysis, there was a statistically significant reduction of 24-h total opioid consumption in patients receiving QLB as compared to the control group (MD: -9.92, 95% CI: -16.35, -3.48 I 2 = 99% p = 0.003). We noted a statistically significant reduction of pain scores in the QLB group as compared to control group at 2-4 h (MD: -0.57, 95% CI: -0.98, -0.17 I 2 = 61% p = 0.005), 6-8 h (MD: -1.45, 95% CI: -2.09, -0.81 I 2 = 86% p < 0.00001), 12 h (MD: -1.12, 95% CI: -1.89, -0.34 I 2 = 93% p = 0.005), 24 h (MD: -0.71, 95% CI: -1.27, -0.15 I 2 = 89% p = 0.01) and 48 h (MD: -0.76, 95% CI: -1.37, -0.16 I 2 = 85% p = 0.01) after the procedure. There was a statistically significant reduction in the risk of nausea/vomiting (RR: 0.40, 95% CI: 0.18, 0.88 I 2 = 62% p = 0.02) in patients receiving QLB but no difference in the risk of pruritis (RR: 0.46, 95% CI: 0.17, 1.24 I 2 = 16% p = 0.13) and urinary retention (RR: 0.44, 95% CI: 0.19, 1.02 I 2 = 0% p = 0.06).
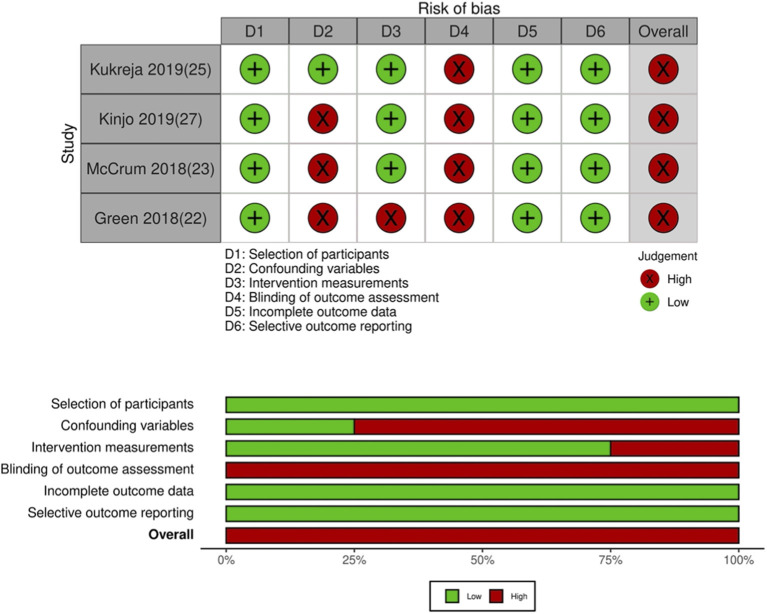
Conclusion: QLB as a part of a multimodal analgesic regimen reduces opioid consumption and pain scores in patients undergoing hip surgeries. The certainty of evidence based on GRADE was moderate. Despite the statistically significant results, the clinical relevance of the analgesic efficacy of QLB is debatable due to the small effect size.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier: CRD42021267861.
Keywords: arthroplasty; arthroscopy; hip surgery; nerve block; pain.
Copyright © 2022 Li, Wei, Huang, Li, Liu, Liu and Jin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources