

Cerebro-Cardiovascular Risk, Target Organ Damage, and Treatment Outcomes in Primary Aldosteronism
- PMID: 35187110
- PMCID: PMC8847442
- DOI: 10.3389/fcvm.2021.798364
Cerebro-Cardiovascular Risk, Target Organ Damage, and Treatment Outcomes in Primary Aldosteronism
Abstract
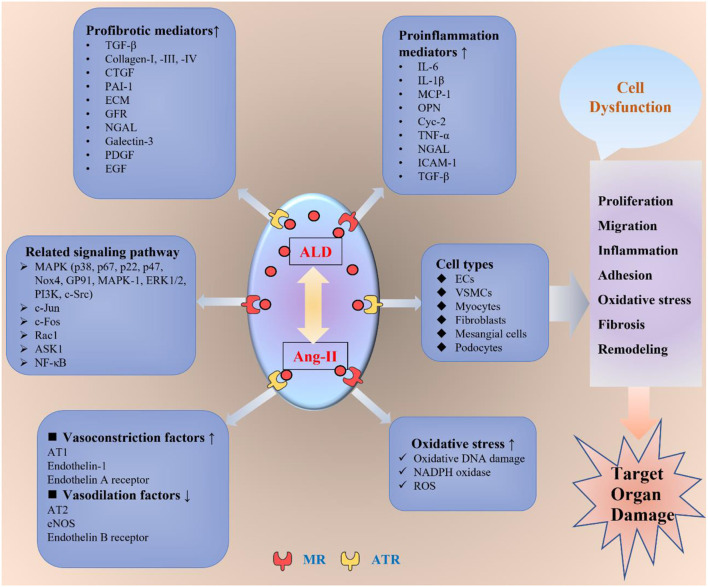
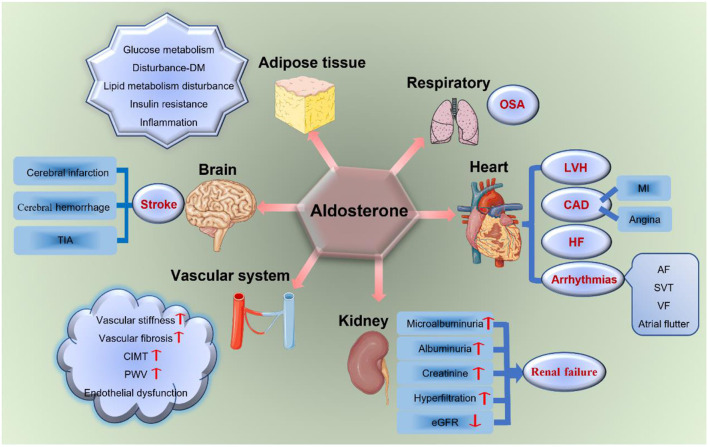
Primary aldosteronism (PA) is the most common type of endocrine hypertension, and numerous experimental and clinical evidence have verified that prolonged exposure to excess aldosterone is responsible for an increased risk of cerebro-cardiovascular events and target organ damage (TOD) in patients with PA. Therefore, focusing on restoring the toxic effects of excess aldosterone on the target organs is very important to reduce cerebro-cardiovascular events. Current evidence convincingly demonstrates that both surgical and medical treatment strategies would benefit cerebro-cardiovascular outcomes and mortality in the long term. Understanding cerebro-cardiovascular risk in PA would help clinical doctors to achieve both early diagnosis and treatment. Therefore, in this review, we will summarize the cerebro-cardiovascular risk in PA, focusing on the TOD of aldosterone, including brain, heart, vascular system, renal, adipose tissues, diabetes, and obstructive sleep apnea (OSA). Furthermore, the various treatment outcomes of adrenalectomy and medical treatment for patients with PA will also be discussed. We hope this knowledge will help improve cerebro-cardiovascular prognosis and reduce the incidence and mortality of cerebro-cardiovascular events in patients with PA.
Keywords: aldosterone; cerebro-cardiovascular risk; mechanism; primary aldosteronism; target organ damage; treatment.
Copyright © 2022 Lin, Ullah, Wu, Xu, Shan, Lei, Yuan and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Parasiliti-Caprino M, Lopez C, Prencipe N, Lucatello B, Settanni F, Giraudo G, et al. Prevalence of primary aldosteronism and association with cardiovascular complications in patients with resistant and refractory hypertension. J Hypertens. (2020) 38:1841–8. 10.1097/HJH.0000000000002441 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources