

Ixekizumab in radiographic axial spondyloarthritis with and without elevated C-reactive protein or positive magnetic resonance imaging
- PMID: 35188180
- PMCID: PMC9629340
- DOI: 10.1093/rheumatology/keac104
Ixekizumab in radiographic axial spondyloarthritis with and without elevated C-reactive protein or positive magnetic resonance imaging
Abstract
Objective: To evaluate response rates at week 16 with ixekizumab in patients with radiographic axial SpA (r-axSpA) and elevated or normal/low baseline inflammation measured by serum CRP or spinal MRI using data from two randomized, double-blind, placebo (PBO)-controlled phase III trials.
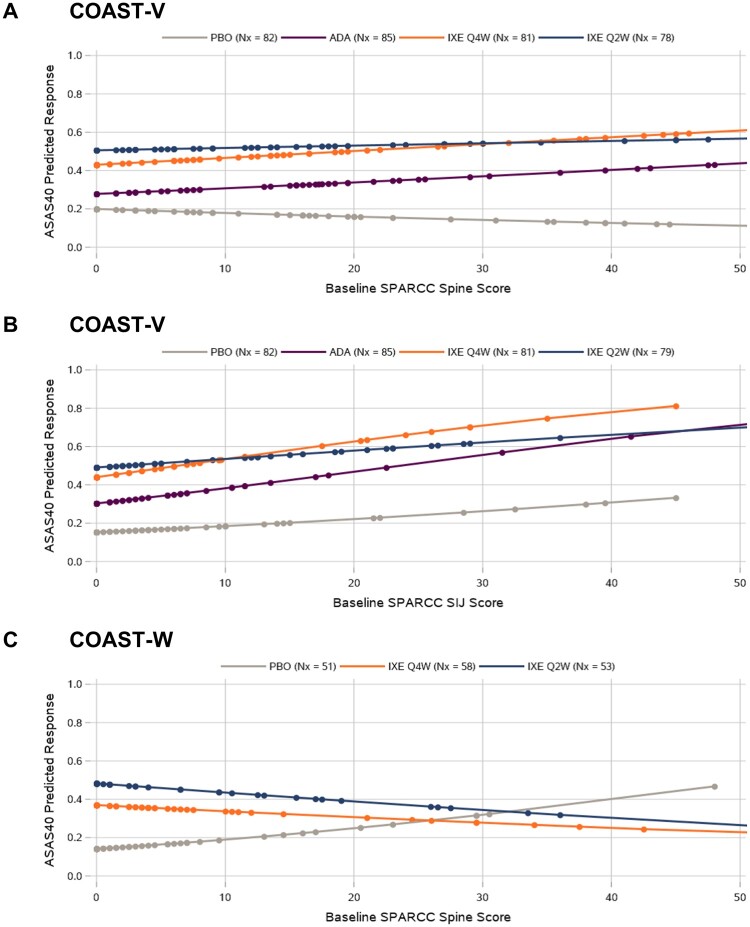
Methods: Biologic-naïve (COAST-V) or TNF inhibitor-experienced (COAST-W) adults with active r-axSpA received 80 mg ixekizumab every 2 weeks (IXEQ2W) or 4 weeks (IXEQ4W) or PBO or active reference [40 mg adalimumab every 2 weeks (ADAQ2W) in COAST-V. At week 16, patients receiving ixekizumab continued as assigned and patients receiving PBO or ADA were rerandomized 1:1 to IXEQ2W or IXEQ4W through week 52. Assessment of SpondyloArthritis international Society 40% (ASAS40) response rates were examined by baseline CRP (≤5 or >5 mg/l) and Spondyloarthritis Research Consortium of Canada (SPARCC) MRI spine inflammation score (<2 or ≥2).
Results: In the COAST-V/W integrated dataset (N = 567), significantly more patients treated with ixekizumab achieved ASAS40 response at week 16 by CRP ≤5 mg/l (27% IXEQ4W, P < 0.05; 35% IXEQ2W, P < 0.01 vs 12% PBO), CRP >5 mg/l (39% IXEQ4W, P < 0.001; 43% IXEQ2W, P < 0.001 vs 17% PBO), SPARCC MRI spine score <2 (40% IXEQ4W P < 0.01, 52% IXEQ2W P < 0.001 vs 16% PBO), and SPARCC MRI spine score ≥2 (44% IXEQ4W P < 0.001, 47% IXEQ2W P < 0.001 vs 19% PBO). ASAS40 response was observed with CRP ≤5 mg/l and SPARCC MRI spine score <2 with IXEQ4W (29%) and was significant with IXEQ2W (48%; P < 0.05) vs PBO (13%).
Conclusion: Ixekizumab demonstrated efficacy in the treatment of AS/r-axSpA in patients with and without elevated CRP or evidence of spinal inflammation on MRI.
Trial registration: ClinicalTrials.gov (https://clinicaltrials.gov): NCT02696785, NCT02696798.
Keywords: AS; CRP; MRI; inflammation; ixekizumab; randomized clinical trials.
© The Author(s) 2022. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures



References
-
- Sieper J, Poddubnyy D.. Axial spondyloarthritis. Lancet 2017;390:73–84. - PubMed
-
- Rudwaleit M, Khan MA, Sieper J.. The challenge of diagnosis and classification in early ankylosing spondylitis: do we need new criteria? Arthritis Rheum 2005;52:1000–8. - PubMed
-
- Ward MM, Deodhar A, Gensler LS. et al. 2019 Update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Rheumatol 2019;71:1599–613. - PMC - PubMed
-
- Dougados M, Baeten D.. Spondyloarthritis. Lancet 2011;377:2127–37. - PubMed
-
- Stolwijk C, van Tubergen A, Castillo-Ortiz JD, Boonen A.. Prevalence of extra-articular manifestations in patients with ankylosing spondylitis: a systematic review and meta-analysis. Ann Rheum Dis 2015;74:65–73. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
