

Dolutegravir dosing for children with HIV weighing less than 20 kg: pharmacokinetic and safety substudies nested in the open-label, multicentre, randomised, non-inferiority ODYSSEY trial
- PMID: 35189082
- PMCID: PMC9046096
- DOI: 10.1016/S2352-3018(21)00292-7
Dolutegravir dosing for children with HIV weighing less than 20 kg: pharmacokinetic and safety substudies nested in the open-label, multicentre, randomised, non-inferiority ODYSSEY trial
Abstract
Background: Dolutegravir-based antiretroviral therapy is a preferred first-line treatment for adults and children living with HIV; however, very little pharmacokinetic data for dolutegravir use are available in young children. We therefore aimed to evaluate dolutegravir dosing and safety in children weighing 3 kg to less than 20 kg by assessing pharmacokinetic parameters and safety data in children taking dolutegravir within the ODYSSEY trial.
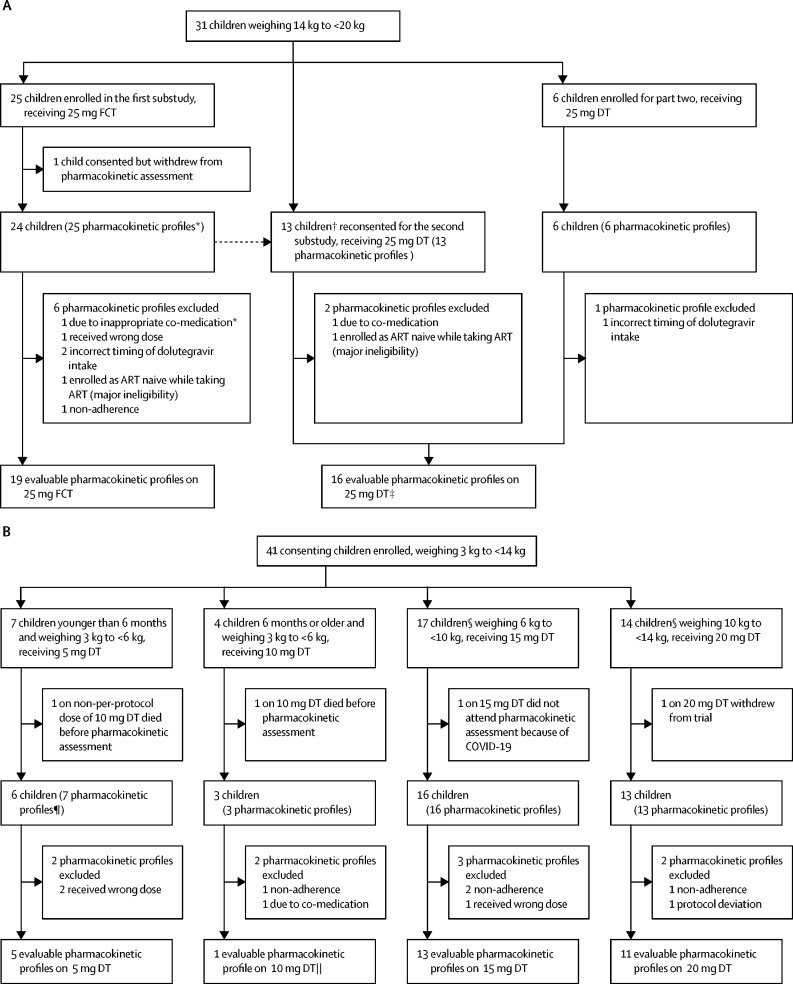
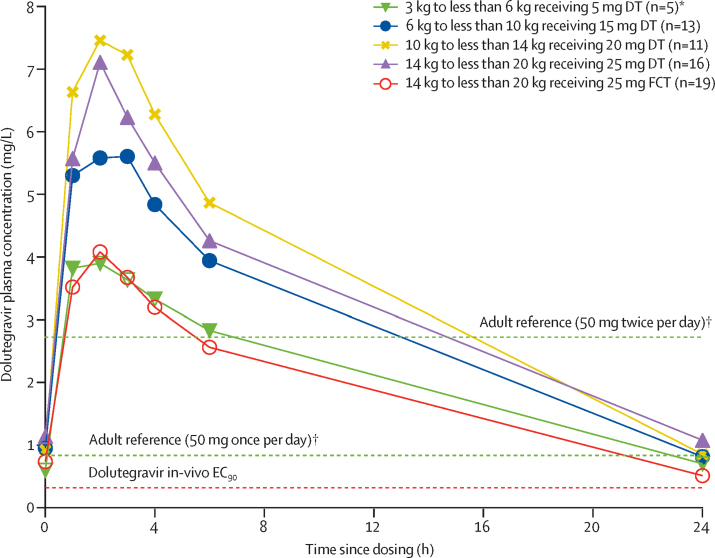
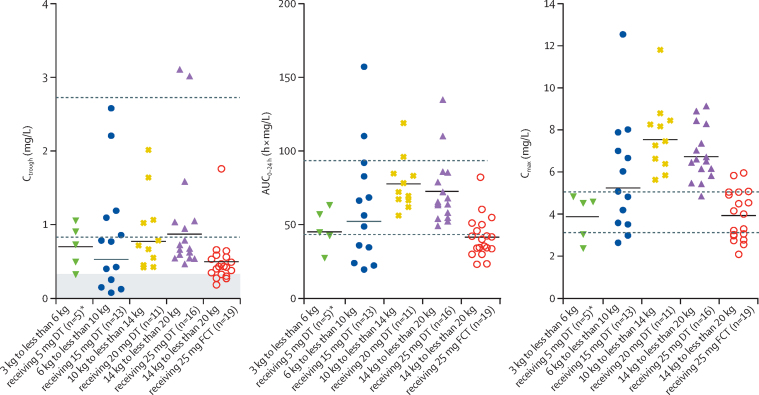
Methods: We did pharmacokinetic substudies nested within the open-label, multicentre, randomised, non-inferiority ODYSSEY trial. We enrolled children from seven research centres in South Africa, Uganda, and Zimbabwe. Children weighing 3 kg to less than 14 kg received 5 mg dispersible tablets of dolutegravir according to WHO weight bands: 5 mg for children weighing 3 kg to less than 6 kg and younger than 6 months, 10 mg for children weighing 3 kg to less than 6 kg and aged 6 months or older, 15 mg for children weighing 6 kg to less than 10 kg, and 20 mg for children weighing 10 kg to less than 14 kg. Children weighing 14 kg to less than 20 kg received a 25 mg film-coated tablet once per day early in the trial or 25 mg dispersible tablets (five 5 mg tablets once per day) later in the trial. A minimum of eight children per weight band or dose was targeted for 24 h pharmacokinetic profiling at steady state. The primary pharmacokinetic parameter was the trough concentration 24 h after observed dolutegravir intake (Ctrough). Pharmacokinetic targets were based on adult dolutegravir Ctrough and the 90% effective concentration (EC90; ie, 0·32 mg/L). Safety was evaluated in eligible children consenting to pharmacokinetic substudies.
Findings: Between May 25, 2017, and Aug 15, 2019, we enrolled 72 children aged between 3 months and 11 years. 71 children were included in the safety population and 55 (76%) of 72 children contributed 65 evaluable pharmacokinetic profiles. Geometric mean Ctrough in children on dispersible tablets in weight bands between 3 kg and less than 20 kg ranged between 0·53-0·87 mg/L, comparable to the adult geometric mean Ctrough of 0·83 mg/L. Variability was high with coefficient of variation percentages ranging between 50% and 150% compared with 26% in adults. Ctrough below EC90 was observed in four (31%) of 13 children weighing 6 kg to less than 10 kg taking 15 mg dispersible tablets, and four (21%) of 19 weighing 14 kg to less than 20 kg taking 25 mg film-coated tablets. The lowest geometric mean Ctrough of 0·44 mg/L was observed in children weighing 14 kg to less than 20 kg on 25 mg film-coated tablets. Exposures were 1·7-2·0 times higher on 25 mg dispersible tablets versus 25 mg film-coated tablets. 19 (27%) of 71 children had 29 reportable grade 3 or higher adverse events (13 serious adverse events, including two deaths), none of which were related to dolutegravir.
Interpretation: Weight-band dosing of paediatric dolutegravir dispersible tablets provides appropriate drug exposure in most children weighing 3 kg to less than 20 kg, with no safety signal. 25 mg film-coated tablets did not achieve pharmacokinetic parameters in children weighing 14 kg to less than 20 kg, which were comparable to adults, suggesting dosing with dispersible tablets is preferable or a higher film-coated tablet dose is required.
Funding: Paediatric European Network for Treatment of AIDS Foundation, ViiV Healthcare, and UK Medical Research Council.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests DMB has received payments for serving on an advisory board of ViiV Healthcare. DMB, PDJB, HW, and AC have received research funding for Radboudumc Institute for Health Sciences from ViiV Healthcare. All other authors declare no competing interests.
Figures
References
-
- UNAIDS Confronting inequalities: lessons for pandemic responses from 40 years of AIDS. 2021. https://www.unaids.org/sites/default/files/media_asset/2021-global-aids-...
-
- UNAIDS Progress towards the start free, stay free, AIDS free targets: 2020 report. 2020. https://www.unaids.org/sites/default/files/media_asset/start-free-stay-f...
-
- WHO . World Health Organization; Geneva: 2019. Update of recommendations on first- and second-line antiretroviral regimens.https://www.who.int/publications/i/item/WHO-CDS-HIV-19.15
-
- Bollen P, Reiss P, Schapiro J, Burger D. Clinical pharmacokinetics and pharmacodynamics of dolutegravir used as a single tablet regimen for the treatment of HIV-1 infection. Expert Opin Drug Saf. 2015;14:1457–1472. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
