Elevated plasma levels of epithelial and endothelial cell markers in COVID-19 survivors with reduced lung diffusing capacity six months after hospital discharge
- PMID: 35189887
- PMCID: PMC8860292
- DOI: 10.1186/s12931-022-01955-5
Elevated plasma levels of epithelial and endothelial cell markers in COVID-19 survivors with reduced lung diffusing capacity six months after hospital discharge
Abstract
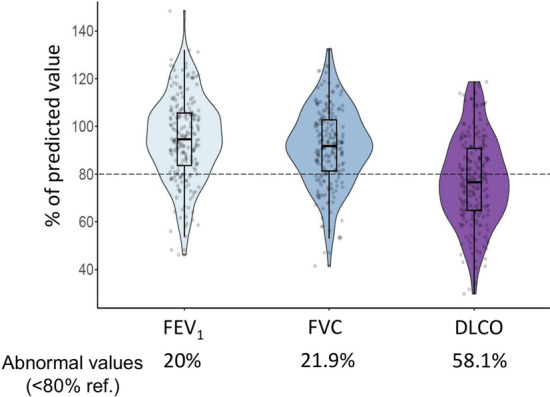
Background: Some COVID-19 survivors present lung function abnormalities during follow-up, particularly reduced carbon monoxide lung diffusing capacity (DLCO). To investigate risk factors and underlying pathophysiology, we compared the clinical characteristics and levels of circulating pulmonary epithelial and endothelial markers in COVID-19 survivors with normal or reduced DLCO 6 months after discharge.
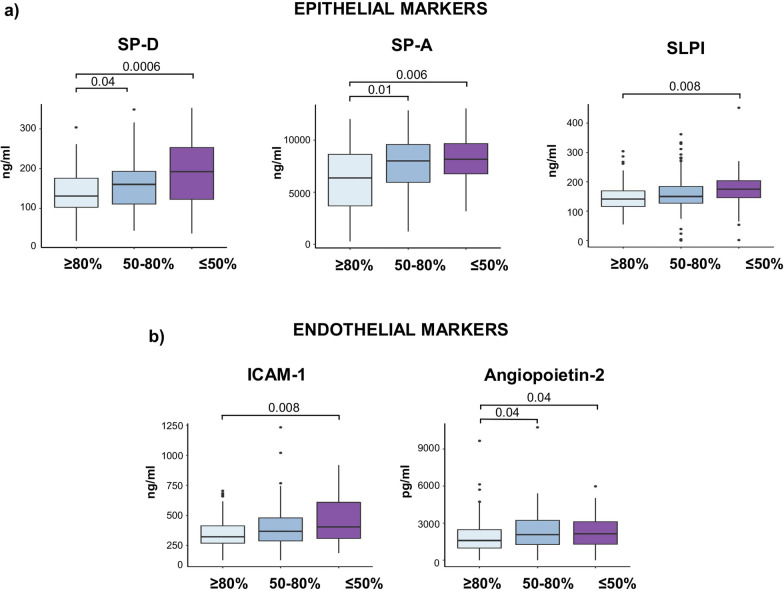
Methods: Prospective, observational study. Clinical characteristics during hospitalization, and spirometry, DLCO and plasma levels of epithelial (surfactant protein (SP) A (SP-A), SP-D, Club cell secretory protein-16 (CC16) and secretory leukocyte protease inhibitor (SLPI)), and endothelial (soluble intercellular adhesion molecule 1 (sICAM-1), soluble E-selectin and Angiopoietin-2) 6 months after hospital discharge were determined in 215 COVID-19 survivors.
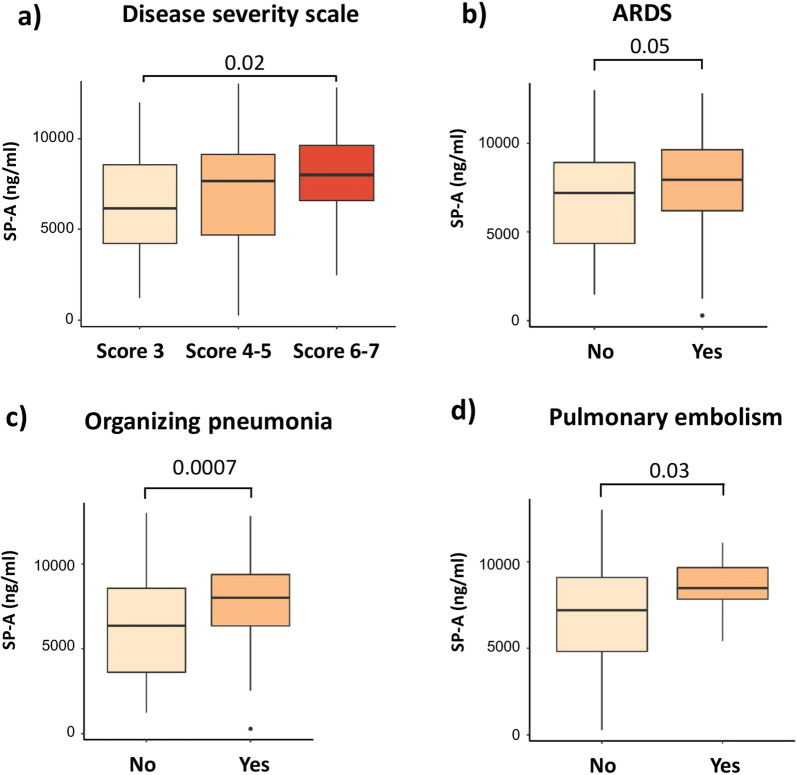
Results: DLCO was < 80% ref. in 125 (58%) of patients, who were older, more frequently smokers, had hypertension, suffered more severe COVID-19 during hospitalization and refer persistent dyspnoea 6 months after discharge. Multivariate regression analysis showed that age ≥ 60 years and severity score of the acute episode ≥ 6 were independent risk factors of reduced DLCO 6 months after discharge. Levels of epithelial (SP-A, SP-D and SLPI) and endothelial (sICAM-1 and angiopoietin-2) markers were higher in patients with reduced DLCO, particularly in those with DLCO ≤ 50% ref. Circulating SP-A levels were associated with the occurrence of acute respiratory distress syndrome (ARDS), organizing pneumonia and pulmonary embolisms during hospitalization.
Conclusions: Reduced DLCO is common in COVID-19 survivors 6 months after hospital discharge, especially in those older than 60 years with very severe acute disease. In these individuals, elevated levels of epithelial and endothelial markers suggest persistent lung damage.
Keywords: DLCO; Endothelial markers; Epithelial markers; Post-COVID; Sequelae.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures