

Change in Left Atrioventricular Coupling Index to Predict Incident Atrial Fibrillation: The Multi-Ethnic Study of Atherosclerosis (MESA)
- PMID: 35191736
- PMCID: PMC9081516
- DOI: 10.1148/radiol.210315
Change in Left Atrioventricular Coupling Index to Predict Incident Atrial Fibrillation: The Multi-Ethnic Study of Atherosclerosis (MESA)
Abstract
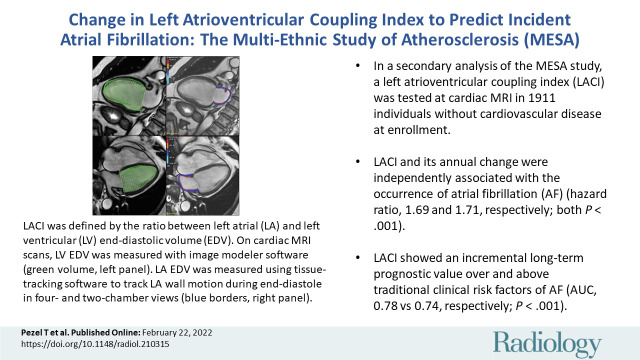
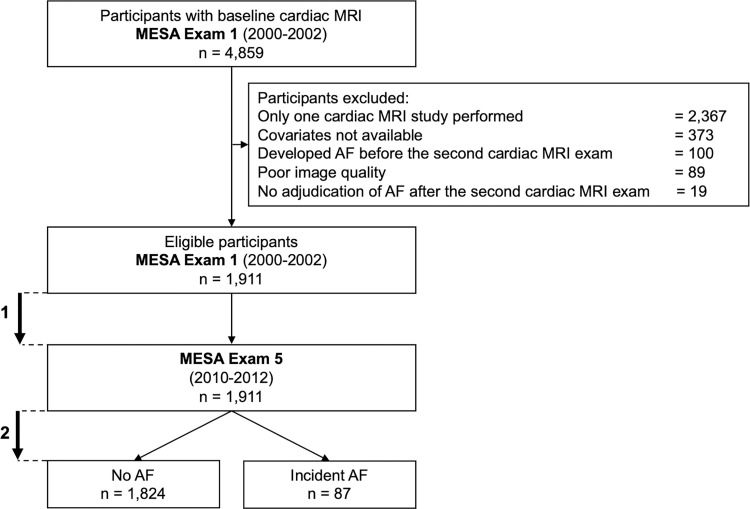
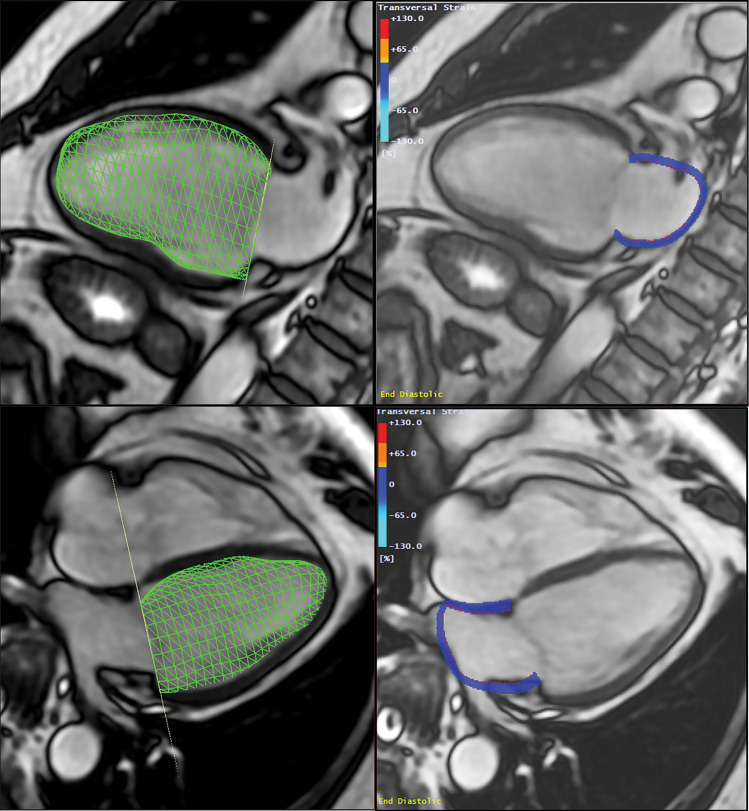
Background Left atrial (LA) and left ventricular (LV) structural and functional parameters have independent prognostic values as predictors of atrial fibrillation (AF). Purpose To investigate the prognostic value of a left atrioventricular coupling index (LACI) and average annualized change in LACI (hereafter, ΔLACI) measured by cardiac MRI to predict incident AF in a population-based sample from the Multi-Ethnic Study of Atherosclerosis (MESA). Materials and Methods In a secondary analysis of the prospective MESA, 1911 study participants without clinically recognized AF and cardiovascular disease at baseline had LACI assessed with cardiac MRI at baseline (examination 1, 2000-2002) and 10 years later (examination 5, 2010-2012). LACI was defined as the ratio of LA to LV end-diastolic volumes. Univariable and multivariable Cox proportional hazard models were used to evaluate the associations of LACI and average ΔLACI with incident AF. Results Among the 1911 participants (mean age, 59 years ± 9 [standard deviation]; 907 men), 87 incident AF events occurred over 3.9 years ± 0.9 after the second imaging (examination 5). After adjustment for traditional risk factors, greater LACI and ΔLACI were independently associated with AF (hazard ratio, 1.69 [95% CI: 1.46, 1.96] and 1.71 [95% CI: 1.50, 1.94], respectively; both P < .001). Adjusted models for LACI and ΔLACI showed improvement in model discrimination compared with currently used AF risk score (Cohort for Heart and Aging Research in Genomic Epidemiology-Atrial Fibrillation, or CHARGE-AF, score) model (area under receiver operating characteristic curve [AUC], 0.78 vs 0.74; and AUC, 0.80 vs 0.74, respectively; both P < .001); and to the final model including individual LA or LV parameters for predicting AF incidence (AUC, 0.78 vs 0.76; and AUC, 0.80 vs 0.78, respectively; both P < .001). Conclusion Atrioventricular coupling (left atrioventricular coupling index [LACI]) and coupling change (annual change in LACI) were strong predictors for atrial fibrillation (AF) in a multiethnic population. Both had incremental prognostic value for predicting AF over traditional risk factors, and superior discrimination compared with the Cohort for Heart and Aging Research in Genomic Epidemiology-Atrial Fibrillation, or CHARGE-AF, score and to individual left atrial or left ventricular parameters. © RSNA, 2022 Online supplemental material is available for this article. See also the editorial by Leiner in this issue.
Conflict of interest statement
Figures
![Kaplan-Meier survival curves for incident atrial fibrillation (AF)
stratified by (A) left atrioventricular coupling index (LACI) terciles and
by (B) a LACI cutoff of 30%. (A) The cumulative hazard was greater in the
third LACI value measured after 10 years (LACI10) tercile compared with the
first tercile for incident AF (hazard ratio [HR], 2.48; 95% CI: 1.53, 3.87;
P < .001). (B) The cumulative hazard was greater for participants
with LACI10 greater than 30% compared with participants with LACI10 of 30%
or less for incident AF (HR, 2.62; 95% CI: 1.72, 4.00; P <
.001).](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/7fcd/9081516/9e06eb67bab6/radiol.210315.fig3.jpg)
![Kaplan-Meier survival curves for incident atrial fibrillation (AF)
stratified by terciles of annual change (Δ) in left atrioventricular
coupling index (LACI) (A) and by annual change in LACI with a cutoff of 1.5%
per year (B). (A) The cumulative hazard was greater in the third tercile
compared with the first tercile for incident AF (hazard ratio [HR], 2.52;
95% CI: 1.57, 3.96; P < .001). (B) The cumulative hazard was greater
for participants with LACI greater than 1.5% per year compared with
participants with annual change in LACI of 1.5% or less per year for
incident AF (HR, 2.77; 95% CI: 1.82, 4.21; P < .001).](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/7fcd/9081516/28dd8fc15490/radiol.210315.fig4.jpg)
![Kaplan-Meier survival curves for incident atrial fibrillation (AF)
stratified simultaneously by left atrioventricular coupling index (LACI)
value measured after 10 years (LACI 10) with a cutoff of 30% and an annual
change (Δ) in LACI with a cutoff of 1.5% per year. In participants
with a LACI10 greater than 30%, the cumulative hazard was greater for
participants with annual change in LACI greater than 1.5% per year than for
those with annual change LACI of 1.5% or less per year (hazard ratio [HR],
2.20; 95% CI: 1.08, 4.15; P < .001). However, among participants with
LACI10 of 30% or less, we found no evidence of differences between those
with annual change in LACI greater than or less than 1.5% per year (HR,
1.19; 95% CI: 0.87, 1.89; P = .46).](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/7fcd/9081516/82983071ebe1/radiol.210315.fig5.jpg)
Comment in
-
Left Atrioventricular Coupling for Early Prediction of Incident Atrial Fibrillation.Radiology. 2022 May;303(2):327-328. doi: 10.1148/radiol.213293. Epub 2022 Feb 22. Radiology. 2022. PMID: 35191742 No abstract available.
Similar articles
-
The Possibilities and Importance of Assessing the Left Atrioventricular Coupling Index Using Various Diagnostic Imaging Methods in an Adult Population: A Comprehensive Review.J Cardiovasc Dev Dis. 2025 Mar 22;12(4):110. doi: 10.3390/jcdd12040110. J Cardiovasc Dev Dis. 2025. PMID: 40278169 Free PMC article. Review.
-
Left Atrioventricular Coupling Index to Predict Incident Heart Failure: The Multi-Ethnic Study of Atherosclerosis.Front Cardiovasc Med. 2021 Sep 1;8:704611. doi: 10.3389/fcvm.2021.704611. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34540915 Free PMC article.
-
Determinants of left atrioventricular coupling index: The Multi-Ethnic Study of Atherosclerosis (MESA).Arch Cardiovasc Dis. 2022 Aug-Sep;115(8-9):414-425. doi: 10.1016/j.acvd.2022.04.011. Epub 2022 Jul 16. Arch Cardiovasc Dis. 2022. PMID: 35906156
-
Prognostic value of a left atrioventricular coupling index in pre- and post-menopausal women from the Multi-Ethnic Study of Atherosclerosis.Front Cardiovasc Med. 2022 Nov 21;9:1066849. doi: 10.3389/fcvm.2022.1066849. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36479563 Free PMC article.
-
The power of the left atrioventricular coupling index in cardiovascular disease.Front Cardiovasc Med. 2025 Apr 10;12:1567856. doi: 10.3389/fcvm.2025.1567856. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40276261 Free PMC article. Review.
Cited by
-
Left and right atrioventricular coupling index in patients with beta-thalassemia major.Int J Cardiovasc Imaging. 2024 Aug;40(8):1631-1640. doi: 10.1007/s10554-024-03146-3. Epub 2024 May 22. Int J Cardiovasc Imaging. 2024. PMID: 38775931
-
The Possibilities and Importance of Assessing the Left Atrioventricular Coupling Index Using Various Diagnostic Imaging Methods in an Adult Population: A Comprehensive Review.J Cardiovasc Dev Dis. 2025 Mar 22;12(4):110. doi: 10.3390/jcdd12040110. J Cardiovasc Dev Dis. 2025. PMID: 40278169 Free PMC article. Review.
-
Differential Stroke Volume between Left and Right Ventricles as a Predictor of Clinical Outcomes: The MESA Study.Radiology. 2024 Jul;312(1):e232973. doi: 10.1148/radiol.232973. Radiology. 2024. PMID: 39041933 Free PMC article.
-
Left Atrial Coupling Index Predicts Heart Failure in Patients with End Stage Renal Disease.Medicina (Kaunas). 2024 Jul 24;60(8):1195. doi: 10.3390/medicina60081195. Medicina (Kaunas). 2024. PMID: 39202477 Free PMC article.
-
Clinical Utility of Atrioventricular Coupling Index in Cardiovascular Disease.J Am Heart Assoc. 2025 Jun 3;14(11):e041392. doi: 10.1161/JAHA.125.041392. Epub 2025 May 22. J Am Heart Assoc. 2025. PMID: 40401599 Free PMC article. Review.
References
-
- Lippi G , Sanchis-Gomar F , Cervellin G . Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge . Int J Stroke 2021. ; 16 ( 2 ): 217 – 221 [Published correction appears in Int J Stroke 2020 Jan 28:1747493020905964]. - PubMed
-
- Virani SS , Alonso A , Benjamin EJ , et al. . Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association . Circulation 2020. ; 141 ( 9 ): e139 – e596 . - PubMed
-
- Chung MK , Eckhardt LL , Chen LY , et al. . Lifestyle and Risk Factor Modification for Reduction of Atrial Fibrillation: A Scientific Statement From the American Heart Association . Circulation 2020. ; 141 ( 16 ): e750 – e772 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
