

Effect of Artificial Intelligence Tutoring vs Expert Instruction on Learning Simulated Surgical Skills Among Medical Students: A Randomized Clinical Trial
- PMID: 35191972
- PMCID: PMC8864513
- DOI: 10.1001/jamanetworkopen.2021.49008
Effect of Artificial Intelligence Tutoring vs Expert Instruction on Learning Simulated Surgical Skills Among Medical Students: A Randomized Clinical Trial
Abstract
Importance: To better understand the emerging role of artificial intelligence (AI) in surgical training, efficacy of AI tutoring systems, such as the Virtual Operative Assistant (VOA), must be tested and compared with conventional approaches.
Objective: To determine how VOA and remote expert instruction compare in learners' skill acquisition, affective, and cognitive outcomes during surgical simulation training.
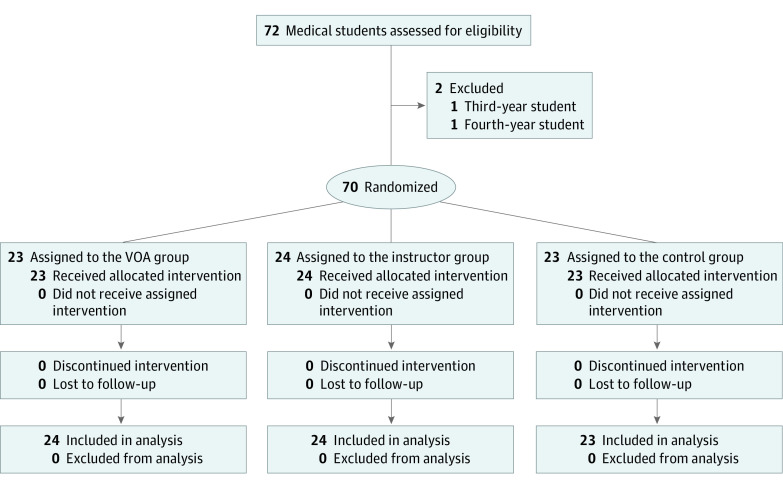
Design, setting, and participants: This instructor-blinded randomized clinical trial included medical students (undergraduate years 0-2) from 4 institutions in Canada during a single simulation training at McGill Neurosurgical Simulation and Artificial Intelligence Learning Centre, Montreal, Canada. Cross-sectional data were collected from January to April 2021. Analysis was conducted based on intention-to-treat. Data were analyzed from April to June 2021.
Interventions: The interventions included 5 feedback sessions, 5 minutes each, during a single 75-minute training, including 5 practice sessions followed by 1 realistic virtual reality brain tumor resection. The 3 intervention arms included 2 treatment groups, AI audiovisual metric-based feedback (VOA group) and synchronous verbal scripted debriefing and instruction from a remote expert (instructor group), and a control group that received no feedback.
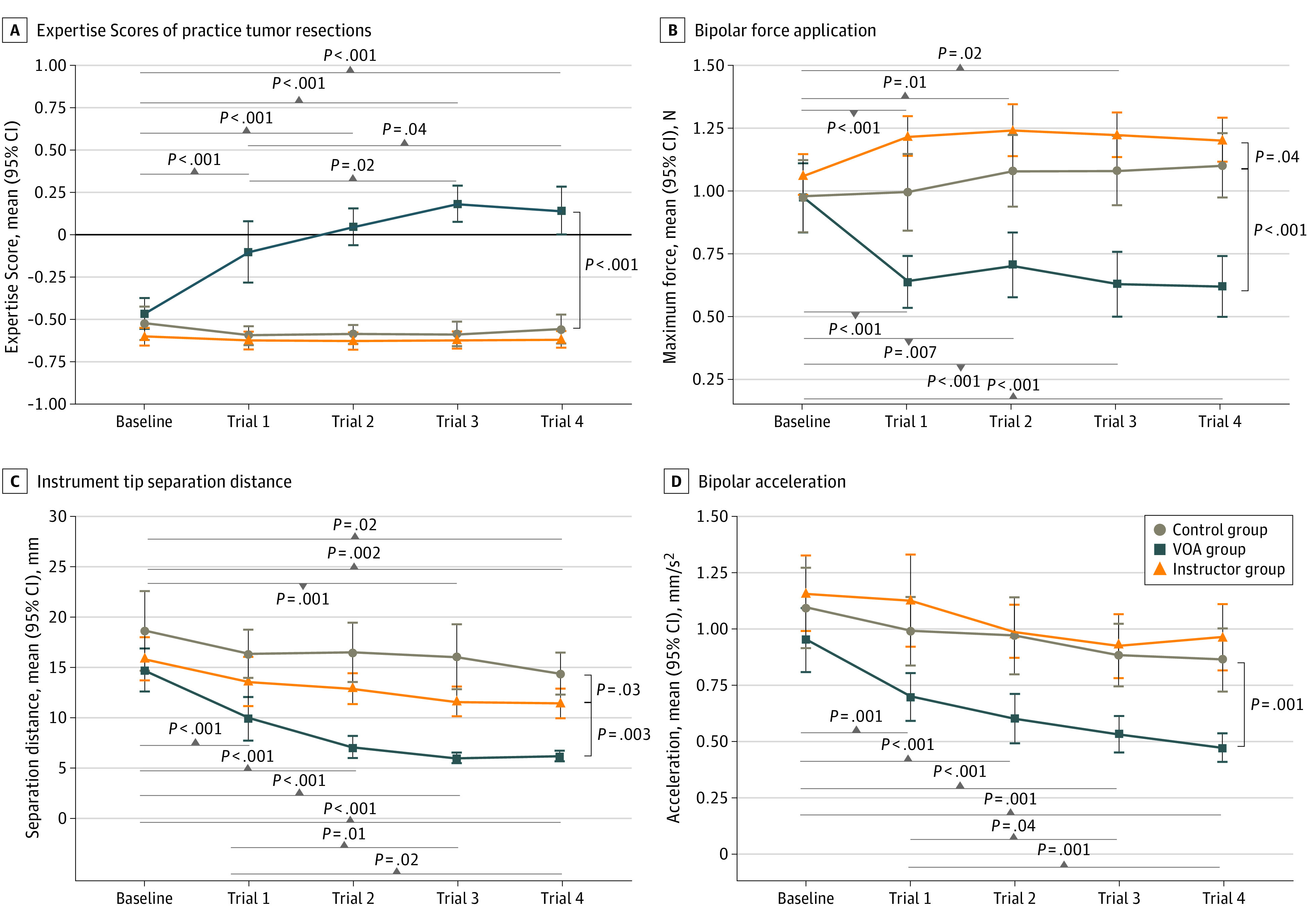
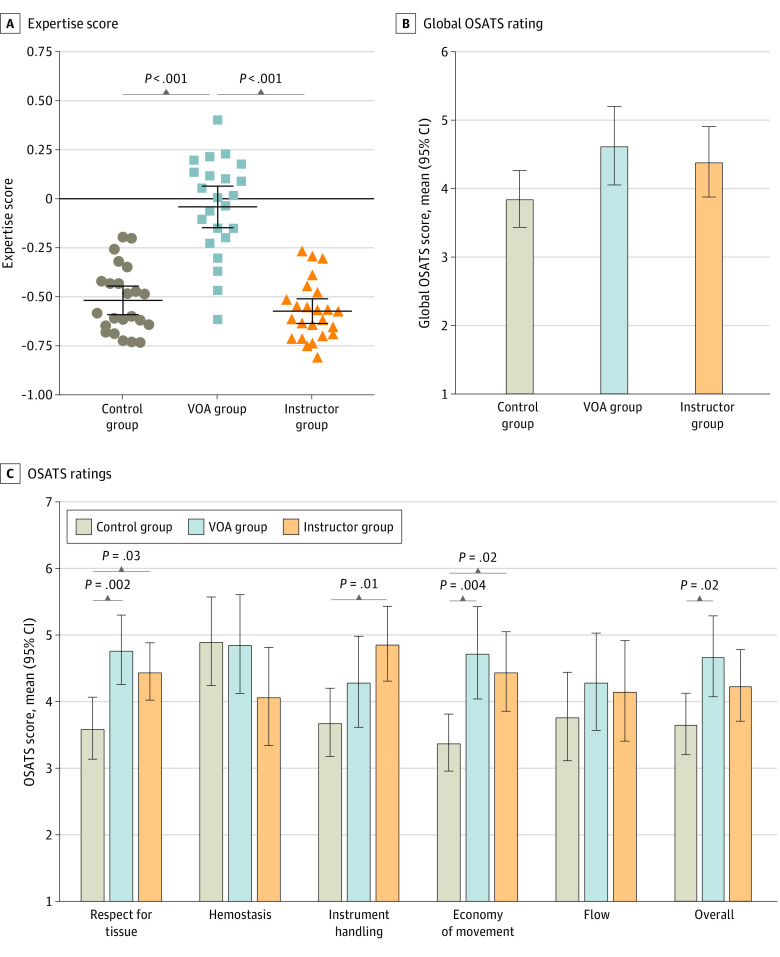
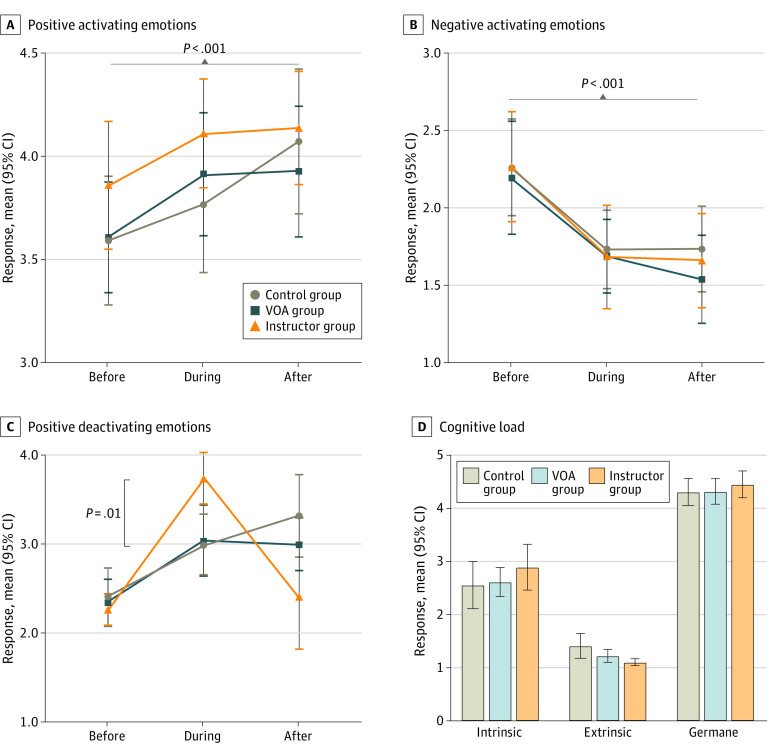
Main outcomes and measures: The coprimary outcomes were change in procedural performance, quantified as Expertise Score by a validated assessment algorithm (Intelligent Continuous Expertise Monitoring System [ICEMS]; range, -1.00 to 1.00) for each practice resection, and learning and retention, measured from performance in realistic resections by ICEMS and blinded Objective Structured Assessment of Technical Skills (OSATS; range 1-7). Secondary outcomes included strength of emotions before, during, and after the intervention and cognitive load after intervention, measured in self-reports.
Results: A total of 70 medical students (41 [59%] women and 29 [41%] men; mean [SD] age, 21.8 [2.3] years) from 4 institutions were randomized, including 23 students in the VOA group, 24 students in the instructor group, and 23 students in the control group. All participants were included in the final analysis. ICEMS assessed 350 practice resections, and ICEMS and OSATS evaluated 70 realistic resections. VOA significantly improved practice Expertise Scores by 0.66 (95% CI, 0.55 to 0.77) points compared with the instructor group and by 0.65 (95% CI, 0.54 to 0.77) points compared with the control group (P < .001). Realistic Expertise Scores were significantly higher for the VOA group compared with instructor (mean difference, 0.53 [95% CI, 0.40 to 0.67] points; P < .001) and control (mean difference. 0.49 [95% CI, 0.34 to 0.61] points; P < .001) groups. Mean global OSATS ratings were not statistically significant among the VOA (4.63 [95% CI, 4.06 to 5.20] points), instructor (4.40 [95% CI, 3.88-4.91] points), and control (3.86 [95% CI, 3.44 to 4.27] points) groups. However, on the OSATS subscores, VOA significantly enhanced the mean OSATS overall subscore compared with the control group (mean difference, 1.04 [95% CI, 0.13 to 1.96] points; P = .02), whereas expert instruction significantly improved OSATS subscores for instrument handling vs control (mean difference, 1.18 [95% CI, 0.22 to 2.14]; P = .01). No significant differences in cognitive load, positive activating, and negative emotions were found.
Conclusions and relevance: In this randomized clinical trial, VOA feedback demonstrated superior performance outcome and skill transfer, with equivalent OSATS ratings and cognitive and emotional responses compared with remote expert instruction, indicating advantages for its use in simulation training.
Trial registration: ClinicalTrials.gov Identifier: NCT04700384.
Conflict of interest statement
Figures
References
-
- Lawrence C. Medical Minds, Surgical Bodies. In: Lawrence C, Shapin S, eds. Science Incarnate: Historical Embodiments of Natural Knowledge. University of Chicago Press; 1998:156-201.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
