

Surgical stabilization versus nonoperative treatment for flail and non-flail rib fracture patterns in patients with traumatic brain injury
- PMID: 35192003
- PMCID: PMC9360098
- DOI: 10.1007/s00068-022-01906-1
Surgical stabilization versus nonoperative treatment for flail and non-flail rib fracture patterns in patients with traumatic brain injury
Abstract
Purpose: Literature on outcomes after SSRF, stratified for rib fracture pattern is scarce in patients with moderate to severe traumatic brain injury (TBI; Glasgow Coma Scale ≤ 12). We hypothesized that SSRF is associated with improved outcomes as compared to nonoperative management without hampering neurological recovery in these patients.
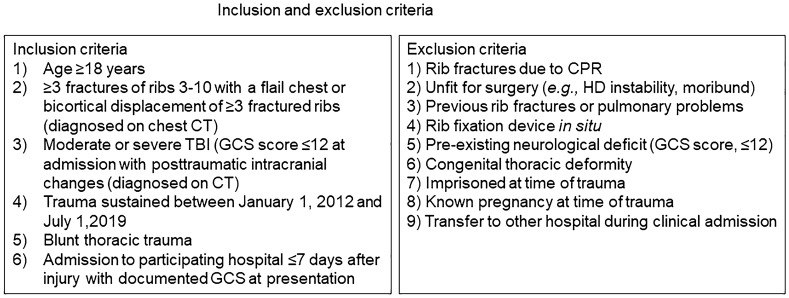
Methods: A post hoc subgroup analysis of the multicenter, retrospective CWIS-TBI study was performed in patients with TBI and stratified by having sustained a non-flail fracture pattern or flail chest between January 1, 2012 and July 31, 2019. The primary outcome was mechanical ventilation-free days and secondary outcomes were in-hospital outcomes. In multivariable analysis, outcomes were assessed, stratified for rib fracture pattern.
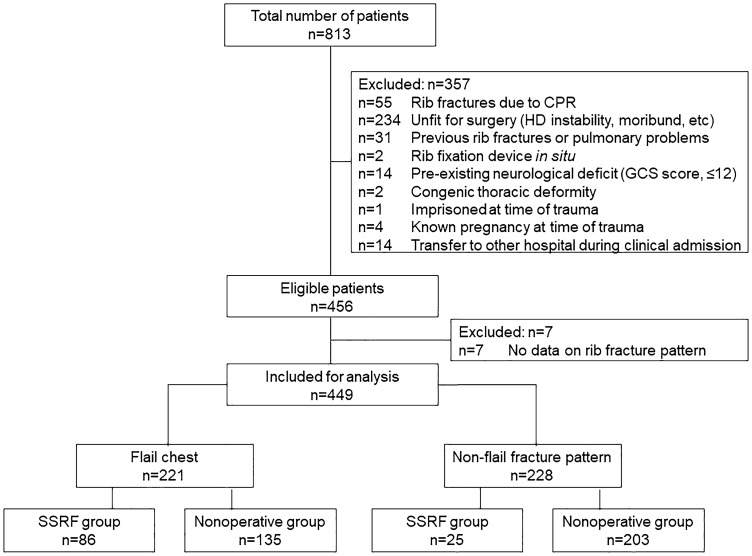
Results: In total, 449 patients were analyzed. In patients with a non-flail fracture pattern, 25 of 228 (11.0%) underwent SSRF and in patients with a flail chest, 86 of 221 (38.9%). In multivariable analysis, ventilator-free days were similar in both treatment groups. For patients with a non-flail fracture pattern, the odds of pneumonia were significantly lower after SSRF (odds ratio 0.29; 95% CI 0.11-0.77; p = 0.013). In patients with a flail chest, the ICU LOS was significantly shorter in the SSRF group (beta, - 2.96 days; 95% CI - 5.70 to - 0.23; p = 0.034).
Conclusion: In patients with TBI and a non-flail fracture pattern, SSRF was associated with a reduced pneumonia risk. In patients with TBI and a flail chest, a shorter ICU LOS was observed in the SSRF group. In both groups, SSRF was safe and did not hamper neurological recovery.
Keywords: Flail chest; Rib fracture; Surgical stabilization of rib fractures; Thoracic trauma; Traumatic brain injury.
© 2022. The Author(s).
Conflict of interest statement
PAC reports grants from DepuySynthes, Stryker, AORF, grants from COTA, AONA, OMeGA, OREF, grants from Zimmer-Biomet, Acumed, personal fees from AO Foundation, other from BoneFoams, Inc, grants from KLS Martin, personal fees from Exactech, personal fees from J&J DepuySynthes, outside the submitted work. ARD is a consultant for Zimmer-Biomet. JDF reports an unrestricted research grant from Varian for an investigator-initiated trial. EAE is a paid speaker for Synthes. SFM receives lecture fees from Johnson & Johnson and Zimmer-Biomet. FMP is part of the teaching faculty for KLS-Martin and Zimmer-Biomet. MMEW and EMMVL report grants from the Netherlands Organization for Health Research and Development (ZonMw), DepuySynthes, Stichting Coolsingel, and Ostheosynthesis and Trauma Care Foundation, outside the submitted work. All other authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
