

Diagnostic accuracy of coronary computed tomography angiography for the evaluation of obstructive coronary artery disease in patients referred for transcatheter aortic valve implantation: a systematic review and meta-analysis
- PMID: 35192010
- PMCID: PMC9279258
- DOI: 10.1007/s00330-022-08603-y
Diagnostic accuracy of coronary computed tomography angiography for the evaluation of obstructive coronary artery disease in patients referred for transcatheter aortic valve implantation: a systematic review and meta-analysis
Abstract
Objective: To evaluate the diagnostic accuracy of coronary computed tomography angiography (CCTA) for the evaluation of obstructive coronary artery disease (CAD) in patients referred for transcatheter aortic valve implantation (TAVI).
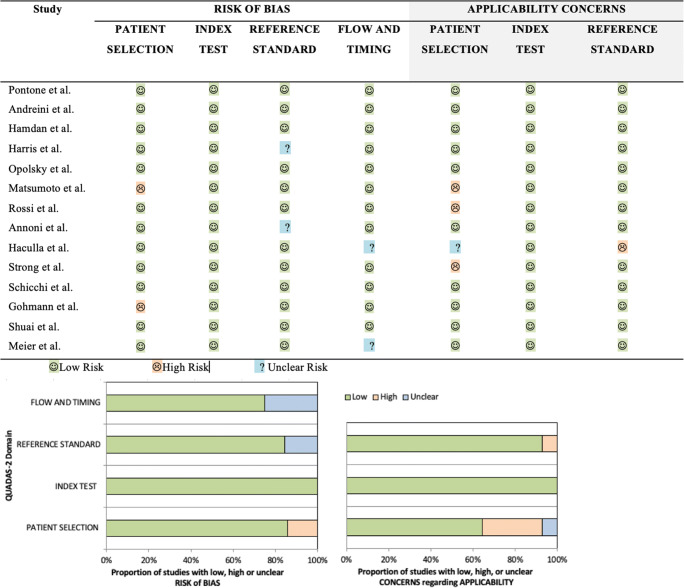
Methods: EMBASE, PubMed/MEDLINE, and CENTRAL were searched for studies reporting accuracy of CCTA for the evaluation of obstructive CAD compared with invasive coronary angiography (ICA) as the reference standard. QUADAS-2 tool was used to assess the risk of bias. A bivariate random effects model was used to analyze, pool, and plot the diagnostic performance measurements across studies. Pooled sensitivity, specificity, positive ( + LR) and negative (-LR) likelihood ratio, diagnostic odds ratio (DOR), and hierarchical summary ROC curve (HSROC) were evaluated. Prospero registration number: CRD42021252527.
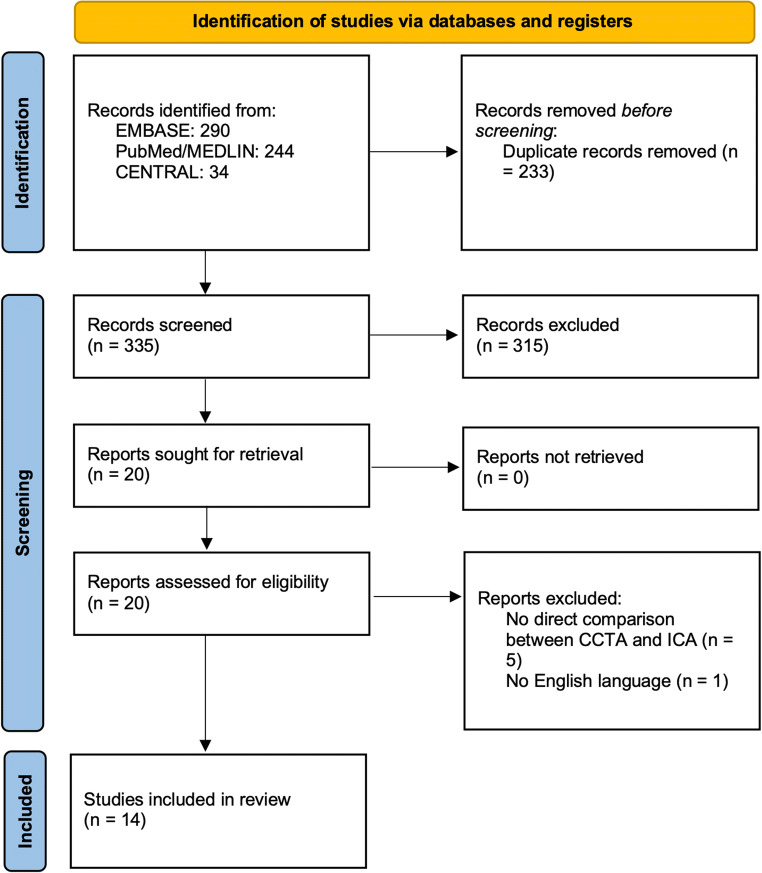
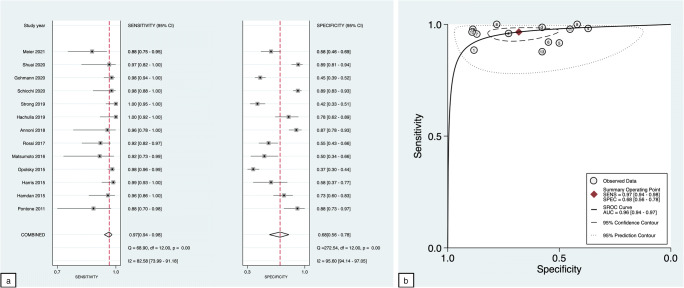
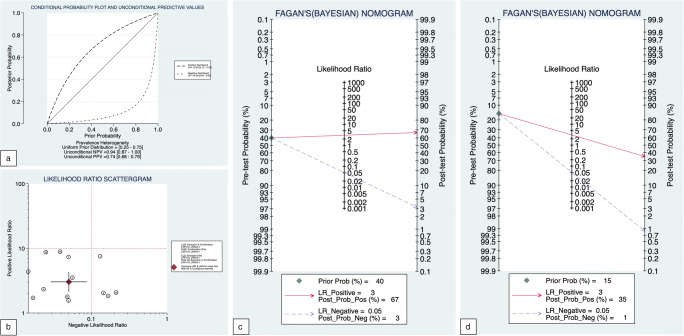
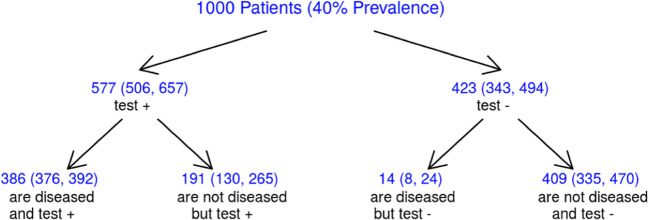
Results: Fourteen studies (2533 patients) were included. In the intention-to-diagnose patient-level analysis, sensitivity and specificity for CCTA were 97% (95% CI: 94-98%) and 68% (95% CI: 56-68%), respectively, and + LR and -LR were 3.0 (95% CI: 2.1-4.3) and 0.05 (95% CI: 0.03 - 0.09), with DOR equal to 60 (95% CI: 30-121). The area under the HSROC curve was 0.96 (95% CI: 0.94-0.98). No significant difference in sensitivity was found between single-heartbeat and other CT scanners (96% (95% CI: 90 - 99%) vs. 97% (95% CI: 94-98%) respectively; p = 0.37), whereas the specificity of single-heartbeat scanners was higher (82% (95% CI: 66-92%) vs. 60% (95% CI: 46 - 72%) respectively; p < 0.0001). Routine CCTA in the pre-TAVI workup could save 41% (95% CI: 34 - 47%) of ICAs if a disease prevalence of 40% is assumed.
Conclusions: CCTA proved an excellent diagnostic accuracy for assessing obstructive CAD in patients referred for TAVI; the use of single-heartbeat CT scanners can further improve these findings.
Key points: • CCTA proved to have an excellent diagnostic accuracy for assessing obstructive CAD in patients referred for TAVI. • Routine CCTA in the pre-TAVI workup could save more than 40% of ICAs. • Single-heartbeat CT scanners had higher specificity than others in the assessment of obstructive CAD in patients referred for TAVI.
Keywords: Aortic valve stenosis; Computed tomography angiography; Coronary artery disease; Transcatheter aortic valve replacement.
© 2022. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
