

Postoperative fluid balance and outcomes after Pancreaticoduodenectomy: a retrospective study in 301 patients
- PMID: 35192049
- PMCID: PMC9283355
- DOI: 10.1007/s00423-022-02443-6
Postoperative fluid balance and outcomes after Pancreaticoduodenectomy: a retrospective study in 301 patients
Abstract
Background: The incidence of postoperative morbidity after pancreaticoduodenectomy (PD) is high; however, whether fluid management after surgery affects postoperative morbidity is unclear. This study aimed to determine whether fluid balance in patients undergoing PD is associated with postoperative complications and mortality.
Methods: Data from a computer-based database of patients who underwent PD between 2016 and 2019 were retrospectively analyzed. Patients were stratified into four quartiles according to their fluid balance at 0-24, 24-48, 48-72, and 72-96 h after surgery. The predefined primary outcome measures were morbidity and mortality rates.
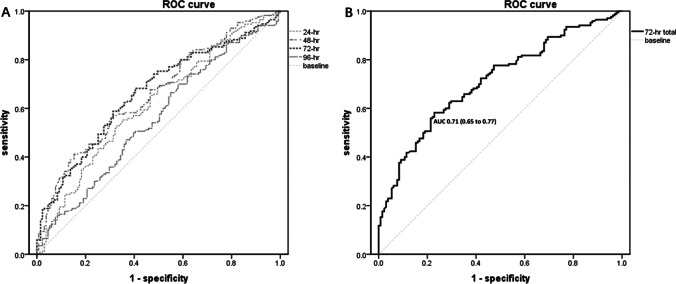
Results: A total of 301 patients were included. The morbidity and mortality rates in the cohort were 56.5% and 3.7%, respectively. The most common complications after PD were postoperative pancreatic fistula (31.9%) and delayed gastric emptying (31.6%). Patients with a higher fluid balance in the 0-24-, 24-48-, and 48-72-h postoperative periods had a higher morbidity rate and longer hospital stay than those with a lower fluid balance (all P < 0.05). Patients with a fluid balance of 4212 mL during the postoperative 0-72 h were most likely to develop complications (P < 0.001). The area under the receiver operating characteristic curve was 0.71 (0.65-0.77), with a sensitivity of 58.24% and a specificity of 77.10%.
Conclusions: Higher postoperative fluid balance seems to be associated with increased morbidity after PD compared to lower fluid balance. Surgeons should pay close attention to the occurrence of complications in patients with a high fluid balance.
Keywords: Fluid management; Outcomes; Pancreaticoduodenectomy; Whipple.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Kimura W, Miyata H, Gotoh M, Hirai I, Kenjo A, Kitagawa Y, et al. A pancreaticoduodenectomy risk model derived from 8575 cases from a national single-race population (Japanese) using a web-based data entry system: the 30-day and in-hospital mortality rates for pancreaticoduodenectomy. Ann Surg. 2014;259(4):773–780. doi: 10.1097/SLA.0000000000000263. - DOI - PubMed
-
- Andrianello S, Marchegiani G, Malleo G, Masini G, Balduzzi A, Paiella S, et al. (2020) Pancreaticojejunostomy with externalized stent vs Pancreaticogastrostomy with externalized stent for patients with high-risk pancreatic anastomosis: a single-center, phase 3, Randomized Clinical Trial. JAMA Surg - PMC - PubMed
-
- Dembinski J, Mariette C, Tuech JJ, Mauvais F, Piessen G, Fuks D, et al. Early removal of intraperitoneal drainage after pancreatoduodenectomy in patients without postoperative fistula at POD3: results of a randomized clinical trial. J Visc Surg. 2019;156(2):103–112. doi: 10.1016/j.jviscsurg.2018.06.006. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
