

Durability of ChAdOx1 nCoV-19 vaccination in people living with HIV
- PMID: 35192543
- PMCID: PMC9057612
- DOI: 10.1172/jci.insight.157031
Durability of ChAdOx1 nCoV-19 vaccination in people living with HIV
Abstract
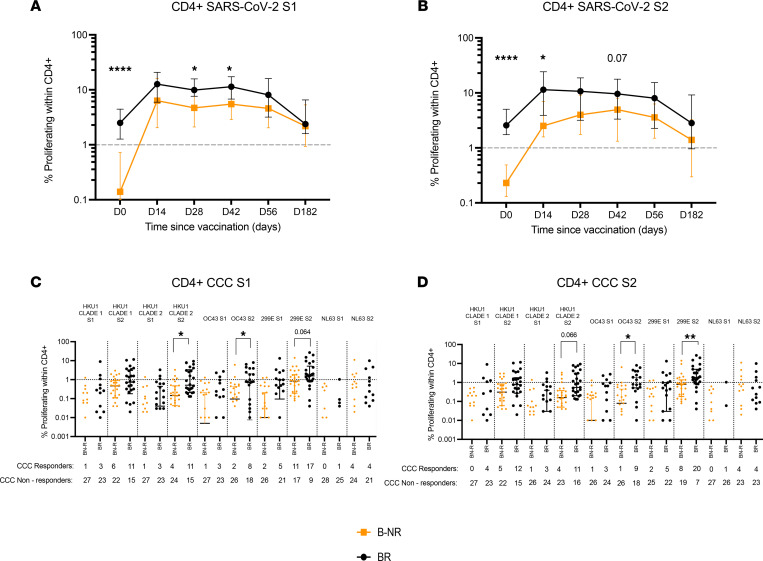
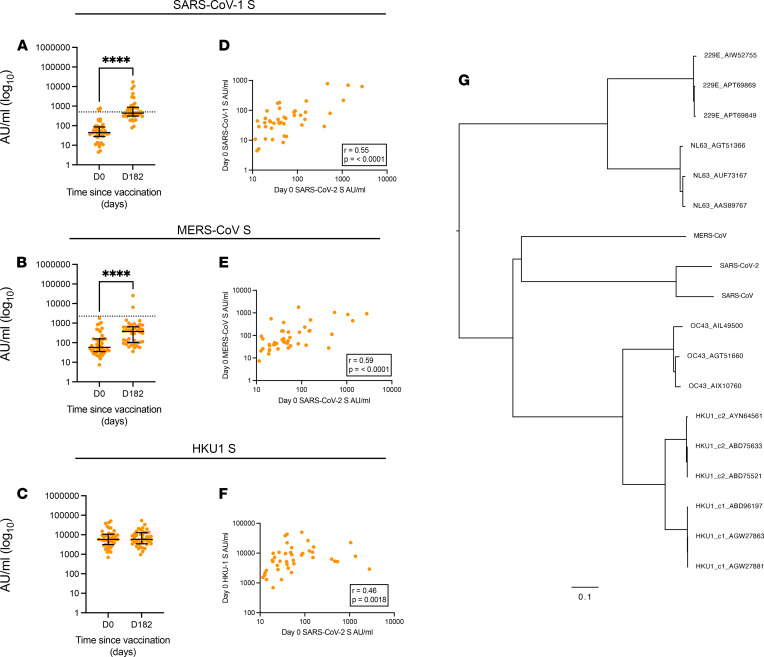
Duration of protection from SARS-CoV-2 infection in people living with HIV (PWH) following vaccination is unclear. In a substudy of the phase II/III the COV002 trial (NCT04400838), 54 HIV+ male participants on antiretroviral therapy (undetectable viral loads, CD4+ T cells > 350 cells/μL) received 2 doses of ChAdOx1 nCoV-19 (AZD1222) 4-6 weeks apart and were followed for 6 months. Responses to vaccination were determined by serology (IgG ELISA and Meso Scale Discovery [MSD]), neutralization, ACE-2 inhibition, IFN-γ ELISpot, activation-induced marker (AIM) assay and T cell proliferation. We show that, 6 months after vaccination, the majority of measurable immune responses were greater than prevaccination baseline but with evidence of a decline in both humoral and cell-mediated immunity. There was, however, no significant difference compared with a cohort of HIV-uninfected individuals vaccinated with the same regimen. Responses to the variants of concern were detectable, although they were lower than WT. Preexisting cross-reactive T cell responses to SARS-CoV-2 spike were associated with greater postvaccine immunity and correlated with prior exposure to beta coronaviruses. These data support the ongoing policy to vaccinate PWH against SARS-CoV-2, and they underpin the need for long-term monitoring of responses after vaccination.
Keywords: AIDS/HIV; Adaptive immunity; COVID-19; Cellular immune response; T cells.
Figures





References
-
- WHO. WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int/ Updated September 17, 2021. Accessed September 17, 2021.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
