

Endothelial Phospholipase Cγ2 Improves Outcomes of Diabetic Ischemic Limb Rescue Following VEGF Therapy
- PMID: 35192691
- PMCID: PMC9044136
- DOI: 10.2337/db21-0830
Endothelial Phospholipase Cγ2 Improves Outcomes of Diabetic Ischemic Limb Rescue Following VEGF Therapy
Abstract
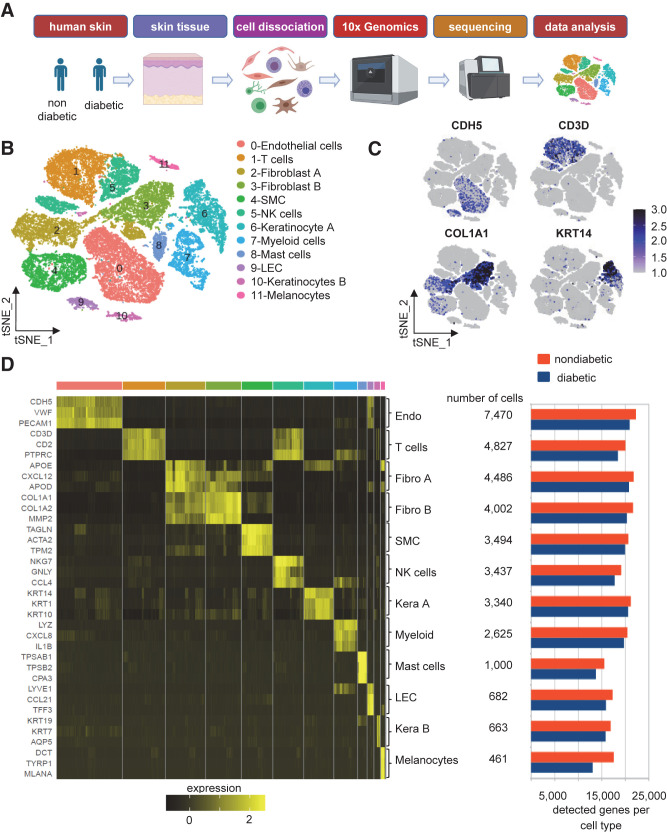
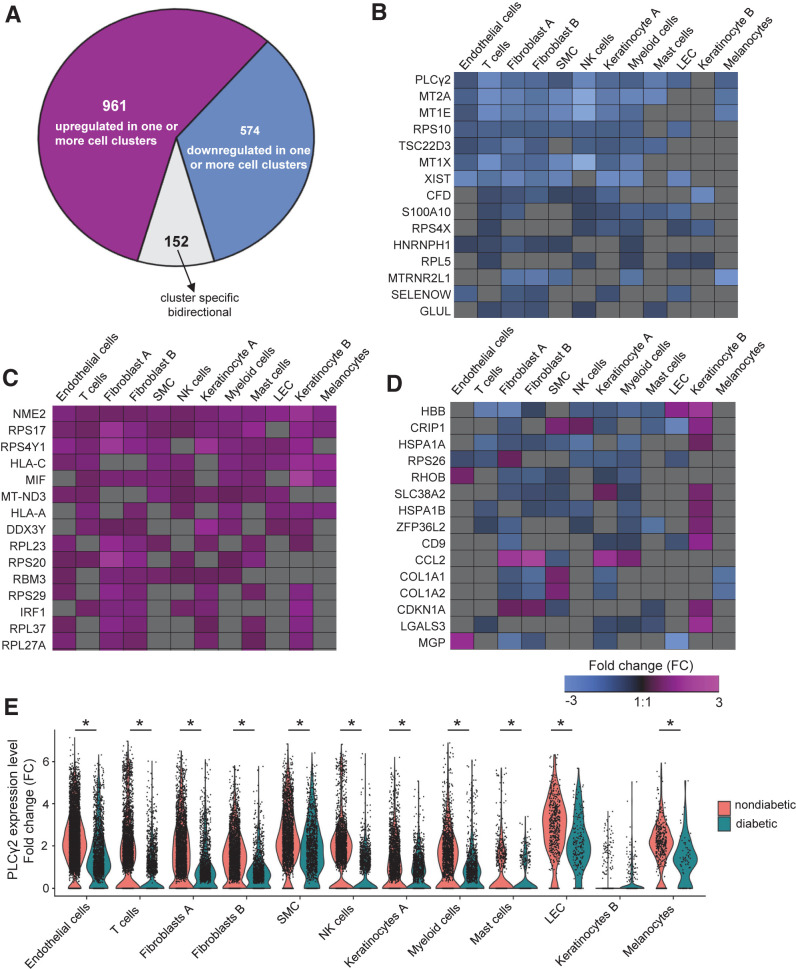
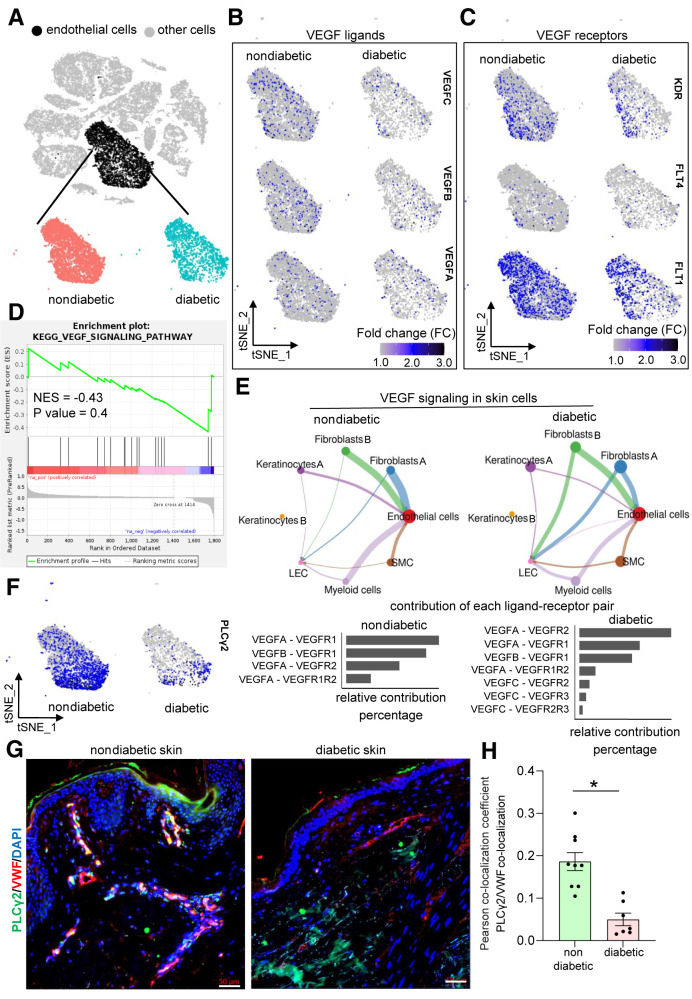
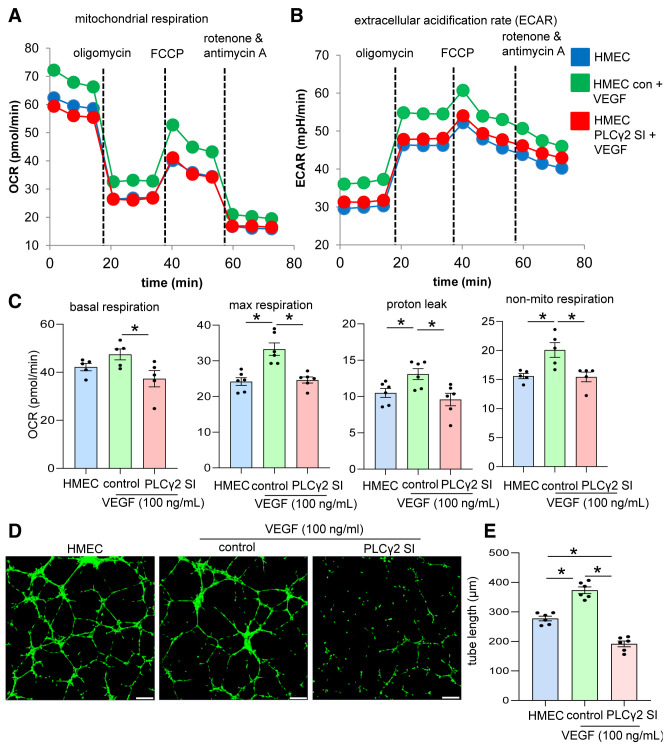
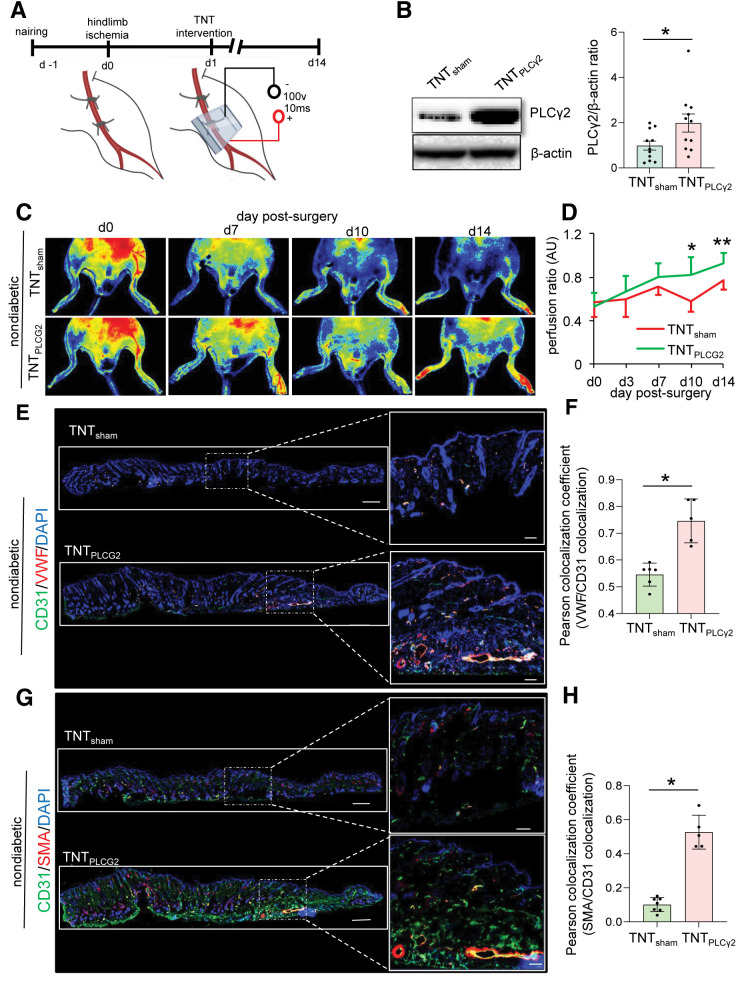
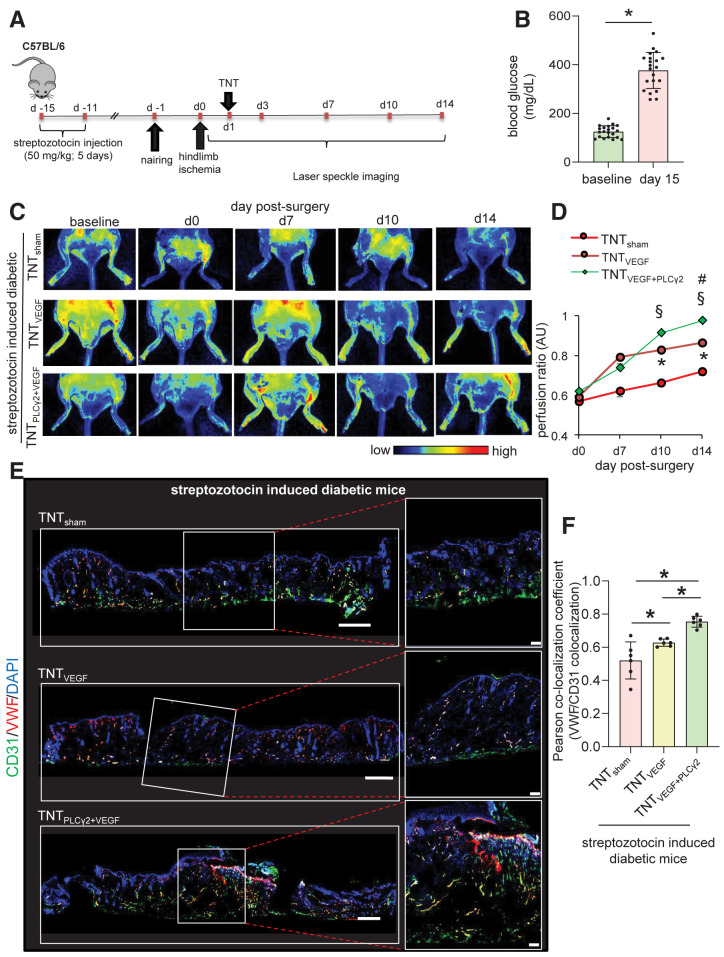
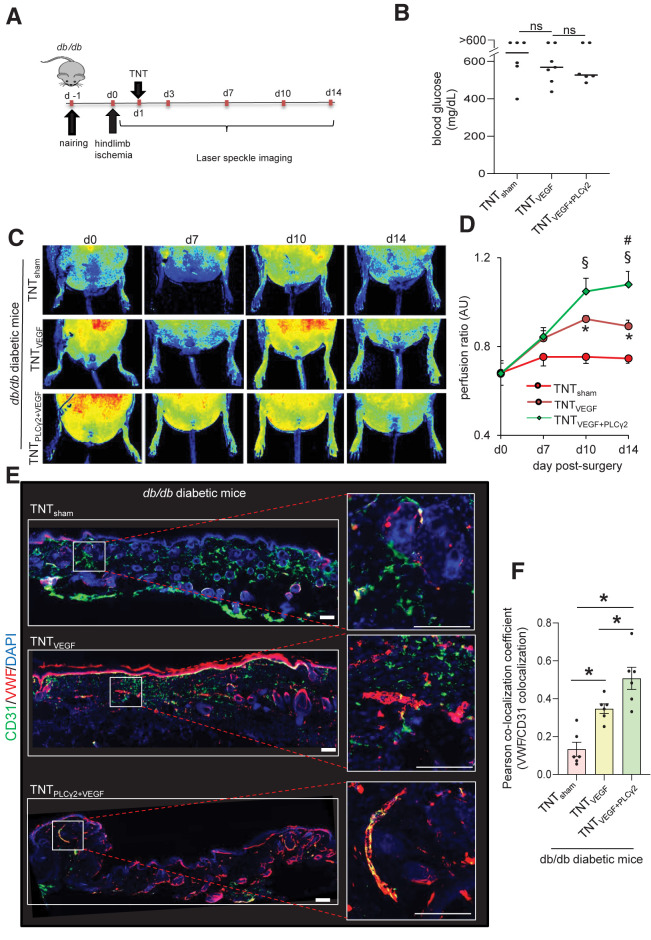
Therapeutic vascular endothelial growth factor (VEGF) replenishment has met with limited success for the management of critical limb-threatening ischemia. To improve outcomes of VEGF therapy, we applied single-cell RNA sequencing (scRNA-seq) technology to study the endothelial cells of the human diabetic skin. Single-cell suspensions were generated from the human skin followed by cDNA preparation using the Chromium Next GEM Single-cell 3' Kit v3.1. Using appropriate quality control measures, 36,487 cells were chosen for downstream analysis. scRNA-seq studies identified that although VEGF signaling was not significantly altered in diabetic versus nondiabetic skin, phospholipase Cγ2 (PLCγ2) was downregulated. The significance of PLCγ2 in VEGF-mediated increase in endothelial cell metabolism and function was assessed in cultured human microvascular endothelial cells. In these cells, VEGF enhanced mitochondrial function, as indicated by elevation in oxygen consumption rate and extracellular acidification rate. The VEGF-dependent increase in cell metabolism was blunted in response to PLCγ2 inhibition. Follow-up rescue studies therefore focused on understanding the significance of VEGF therapy in presence or absence of endothelial PLCγ2 in type 1 (streptozotocin-injected) and type 2 (db/db) diabetic ischemic tissue. Nonviral topical tissue nanotransfection technology (TNT) delivery of CDH5 promoter-driven PLCγ2 open reading frame promoted the rescue of hindlimb ischemia in diabetic mice. Improvement of blood flow was also associated with higher abundance of VWF+/CD31+ and VWF+/SMA+ immunohistochemical staining. TNT-based gene delivery was not associated with tissue edema, a commonly noted complication associated with proangiogenic gene therapies. Taken together, our study demonstrates that TNT-mediated delivery of endothelial PLCγ2, as part of combination gene therapy, is effective in diabetic ischemic limb rescue.
© 2022 by the American Diabetes Association.
Figures
References
-
- Spreen MI, Gremmels H, Teraa M, et al.; PADI and JUVENTAS Study Groups . Diabetes is associated with decreased limb survival in patients with critical limb ischemia: pooled data from two randomized controlled trials. Diabetes Care 2016;39:2058–2064 - PubMed
-
- Lüscher TF, Creager MA, Beckman JA, Cosentino F. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part II. Circulation 2003;108:1655–1661 - PubMed
-
- Abbott RD, Brand FN, Kannel WB. Epidemiology of some peripheral arterial findings in diabetic men and women: experiences from the Framingham Study. Am J Med 1990;88:376–381 - PubMed
-
- Jude EB, Oyibo SO, Chalmers N, Boulton AJ. Peripheral arterial disease in diabetic and nondiabetic patients: a comparison of severity and outcome. Diabetes Care 2001;24:1433–1437 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
