

Outcomes of Patients With Unfavorable Intermediate-Risk Prostate Cancer Treated With External-Beam Radiotherapy Versus Brachytherapy Alone
- PMID: 35193114
- PMCID: PMC9393200
- DOI: 10.6004/jnccn.2021.7061
Outcomes of Patients With Unfavorable Intermediate-Risk Prostate Cancer Treated With External-Beam Radiotherapy Versus Brachytherapy Alone
Abstract
Background: The NCCN Guidelines for Prostate Cancer currently recommend several definitive radiotherapy (RT) options for men with unfavorable intermediate-risk (UIR) prostate cancer: external-beam RT (EBRT) plus androgen deprivation therapy (ADT) or EBRT plus brachytherapy boost with or without ADT. However, brachytherapy alone with or without ADT is not well defined and is currently not recommended for UIR prostate cancer. We hypothesized that men treated with brachytherapy with or without ADT have comparable survival rates to men treated with EBRT with or without ADT.
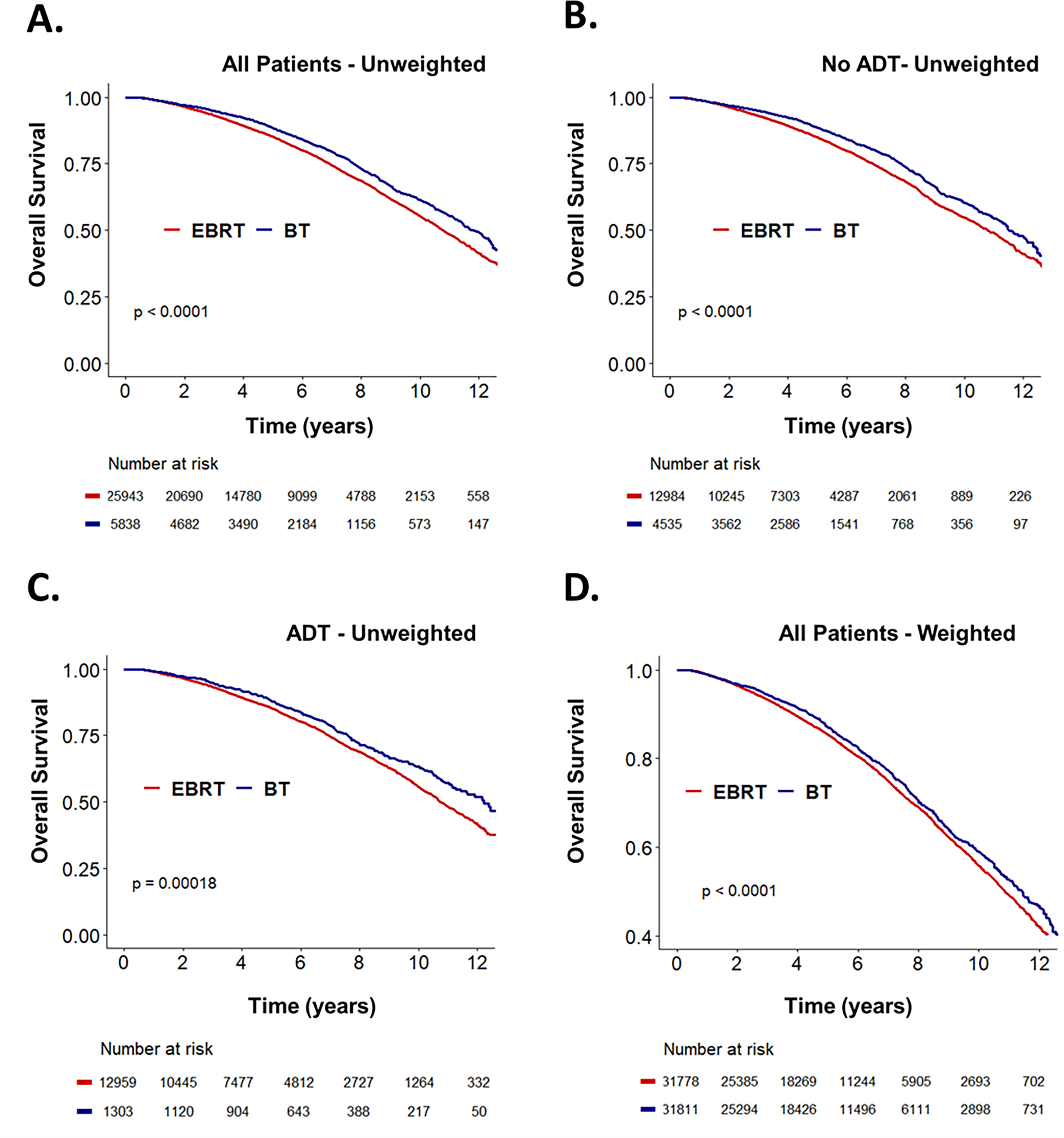
Methods: A total of 31,783 men diagnosed between 2004 and 2015 with UIR prostate cancer were retrospectively reviewed from the National Cancer Database. Men were stratified into 4 groups: EBRT (n=12,985), EBRT plus ADT (n=12,960), brachytherapy (n=4,535), or brachytherapy plus ADT (n=1,303). Inverse probability of treatment weighting (IPTW) was used to adjust for covariable imbalances, and weight-adjusted multivariable analysis (MVA) using Cox regression modeling was used to compare overall survival (OS) hazard ratios (HRs).
Results: Relative to EBRT alone, the following treatments were associated with improved OS: EBRT plus ADT (HR, 0.92; 95% CI, 0.87-0.97; P=.002), brachytherapy alone (HR, 0.90; 95% CI, 0.83-0.98; P=.01), and brachytherapy plus ADT (HR, 0.78; 95% CI, 0.69-0.88; P=.00006). Brachytherapy correlated with improved OS relative to EBRT in men who were not treated with ADT (HR, 0.92; 95% CI, 0.84-0.99; P=.03) and in those receiving ADT (HR, 0.84; 95% CI, 0.75-0.95; P=.004). At 10-year follow-up, 56% and 63% of men receiving EBRT and brachytherapy, respectively, were alive (P<.0001). IPTW was used to determine the average treatment effect of definitive brachytherapy. Relative to EBRT, definitive brachytherapy correlated with improved OS (HR, 0.90; 95% CI, 0.84-0.97; P=.009) on weight-adjusted MVA.
Conclusions: Definitive brachytherapy was associated with improved OS compared with EBRT. The addition of ADT to both EBRT and definitive brachytherapy was associated with improved OS. These results suggest that definitive brachytherapy should be considered as an option for men with UIR prostate cancer.
Figures
Similar articles
-
Assessing the impact of brachytherapy boost and androgen deprivation therapy on survival outcomes for patients with unfavorable intermediate-risk prostate cancer patients treated with external beam radiotherapy.Brachytherapy. 2022 Sep-Oct;21(5):617-625. doi: 10.1016/j.brachy.2022.04.001. Epub 2022 May 28. Brachytherapy. 2022. PMID: 35641370 Free PMC article.
-
Assessing the role of external beam radiation therapy in combination with brachytherapy versus brachytherapy alone for unfavorable intermediate-risk prostate cancer.Brachytherapy. 2022 May-Jun;21(3):317-324. doi: 10.1016/j.brachy.2021.12.008. Epub 2022 Feb 3. Brachytherapy. 2022. PMID: 35123889 Free PMC article.
-
Overall survival comparison between androgen deprivation therapy (ADT) plus external beam radiation therapy (EBRT) vs ADT plus EBRT with brachytherapy boost in clinically node-positive prostate cancer.Brachytherapy. 2020 Sep-Oct;19(5):557-566. doi: 10.1016/j.brachy.2020.05.007. Epub 2020 Jul 3. Brachytherapy. 2020. PMID: 32624405
-
American Brachytherapy Society Task Group Report: Use of androgen deprivation therapy with prostate brachytherapy-A systematic literature review.Brachytherapy. 2017 Mar-Apr;16(2):245-265. doi: 10.1016/j.brachy.2016.11.017. Epub 2017 Jan 16. Brachytherapy. 2017. PMID: 28110898 Free PMC article. Review.
-
Brachytherapy boost (BT-boost) or stereotactic body radiation therapy boost (SBRT-boost) for high-risk prostate cancer (HR-PCa).Cancer Radiother. 2021 Jun;25(4):400-409. doi: 10.1016/j.canrad.2020.11.004. Epub 2021 Jan 18. Cancer Radiother. 2021. PMID: 33478838
Cited by
-
Impact of androgen deprivation therapy in patients with unfavorable intermediate-risk prostate cancer receiving brachytherapy-based dose-escalated radiation therapy.J Contemp Brachytherapy. 2024 Aug;16(4):268-272. doi: 10.5114/jcb.2024.143130. Epub 2024 Sep 12. J Contemp Brachytherapy. 2024. PMID: 39628817 Free PMC article.
-
Ultra-low dose rate brachytherapy (uLDR-BT) in treatment of patients with unfavorable intermediate-risk group prostate cancer - retrospective analysis.Rep Pract Oncol Radiother. 2024 Dec 4;29(5):600-605. doi: 10.5603/rpor.103135. eCollection 2024. Rep Pract Oncol Radiother. 2024. PMID: 39759559 Free PMC article.
References
-
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Prostate Cancer (Version 2.2021). https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf. Accessed March 2, 2021.
-
- Zumsteg ZS, Spratt DE, Pei I, et al. A new risk classification system for therapeutic decision making with intermediate-risk prostate cancer patients undergoing dose-escalated external-beam radiation therapy. Eur Urol. 2013;64(6):895–902. - PubMed
-
- D’Amico AV, Chen MH, Renshaw AA, Loffredo M, Kantoff PW. Androgen suppression and radiation vs radiation alone for prostate cancer: a randomized trial. JAMA. 2008;299(3):289–295. - PubMed
-
- Jones CU, Hunt D, McGowan DG, et al. Radiotherapy and short-term androgen deprivation for localized prostate cancer. N Engl J Med. 2011;365(2):107–118. - PubMed
-
- Pickles T, Morris WJ, Keyes M. High-intermediate prostate cancer treated with low-dose-rate brachytherapy with or without androgen deprivation therapy. Brachytherapy. 2017;16(6):1101–1105. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
