

Anatomical and Technical Considerations of Robot-Assisted Cervical Pedicle Screw Placement: A Cadaveric Study
- PMID: 35195035
- PMCID: PMC10556891
- DOI: 10.1177/21925682211068410
Anatomical and Technical Considerations of Robot-Assisted Cervical Pedicle Screw Placement: A Cadaveric Study
Abstract
Study design: Cadaver study.
Objectives: Assess the feasibility of robot-assisted cervical pedicle screw (RA-CPS) placement and understand the anatomical considerations of this technique.
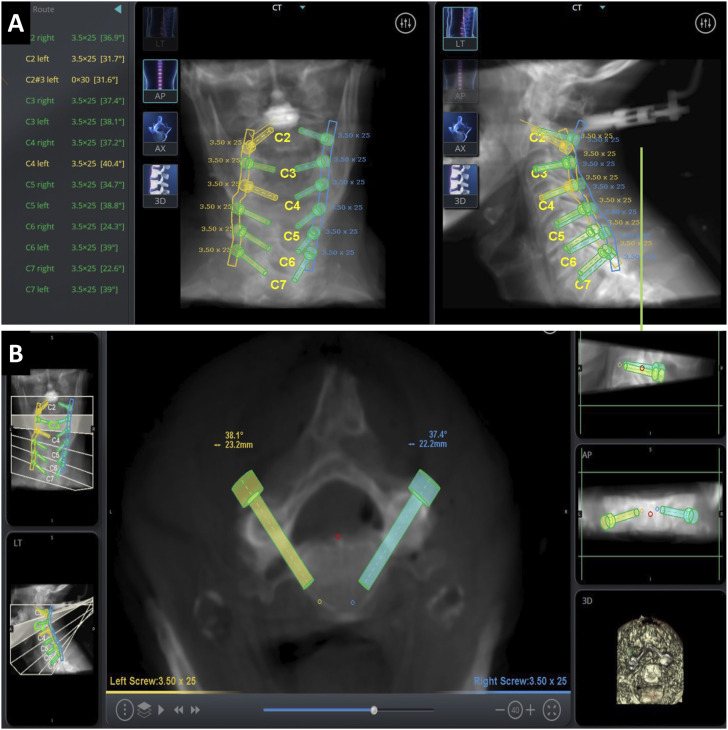
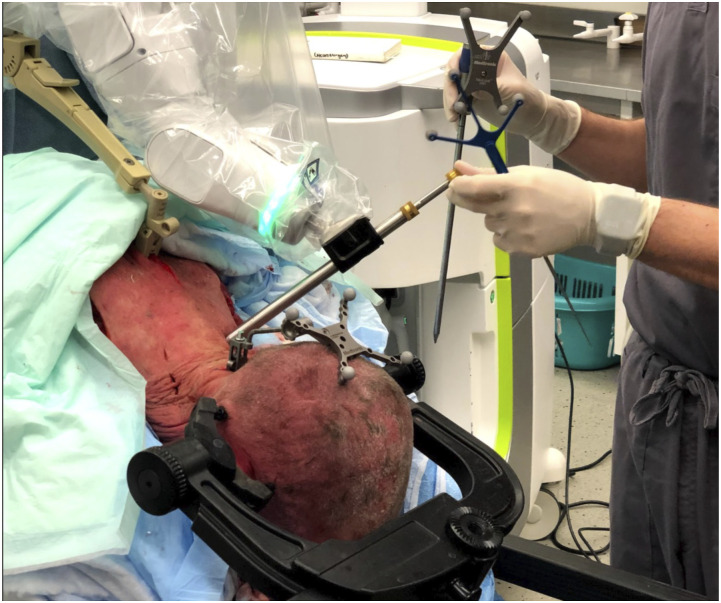
Methods: Four cadaver specimens free from bony pathology were acquired. Anatomical considerations, such as pedicle width (PW) and height (PH), transverse pedicle angle (TPA), and maximal screw length (MSL), were recorded from preoperative computational tomography (CT) scans. Intraoperative cone-beam CT was acquired and registered to the robotic system. After cervical levels were segmented, screw sizes and trajectories were planned, and RA-CPS were placed. Accuracy was assessed using Gertzbein and Robbin's classification on postoperative CT scans.
Results: Thirty-five RA-CPS were placed. Major breaches (≥Grade C) occurred in 28.57% screws. Grade A or B accuracy was found in 71.43% of screws, with the most common direction of breach being medial (81.3%). The greatest proportion of breach per level occurred in the upper subaxial levels, (C3:71.4%, C4 66.6%, C5:50%) which had the smallest PW (C3: 4.34 ± .96 mm, C4: 4.48 ± .60, C5: 5.76 ± 1.11). PH was greatest at C2 (8.14 ± 1.89 mm) and ranged subaxial from 6.36 mm (C3) to 7.48 mm (C7). The mean PW was 5.37 mm and increased caudally from 4.34 mm (C3) to 6.31 mm (C7). The mean TPA was 39.9° and decreased moving caudally 46.9°) to C7 (34.4°). The MSL was 37.1 mm and increased from C2 (26.3 mm) to C7 (41.0 mm).
Conclusion: RA-CPS has the potential to be feasible, but technological and instrument modifications are necessary to increase the accuracy in the cervical region.
Keywords: anatomical; cadaver; cervical pedicle screw; robot-assisted; technical.
Figures
References
-
- Kosmopoulos V, Schizas C. Pedicle screw placement accuracy: a meta-analysis. Spine. 2007;32(3):E111-E120. - PubMed
-
- Fatima N, Massaad E, Hadzipasic M, Shankar GM, Shin JH. Safety and accuracy of robot-assisted placement of pedicle screws compared to conventional free-hand technique: a systematic review and meta-analysis. Spine J. 2020. - PubMed
-
- Khan A, Meyers JE, Siasios I, Pollina J. Next-Generation Robotic Spine Surgery: First Report on Feasibility, Safety, and Learning Curve. Oper Neurosurg (Hagerstown). 2019;17(1):61-69. - PubMed
-
- Hyun SJ, Kim KJ, Jahng TA, Kim HJ. Minimally Invasive Robotic Versus Open Fluoroscopic-guided Spinal Instrumented Fusions: A Randomized Controlled Trial. Spine. 2017;42(6):353-358. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
