

Exercise Intolerance in Facioscapulohumeral Muscular Dystrophy
- PMID: 35195100
- PMCID: PMC9117420
- DOI: 10.1249/MSS.0000000000002882
Exercise Intolerance in Facioscapulohumeral Muscular Dystrophy
Abstract
Purpose: Determine 1) if adults with facioscapulohumeral muscular dystrophy (FSHD) exhibit exercise intolerance and 2) potential contributing mechanisms to exercise intolerance, specific to FSHD.
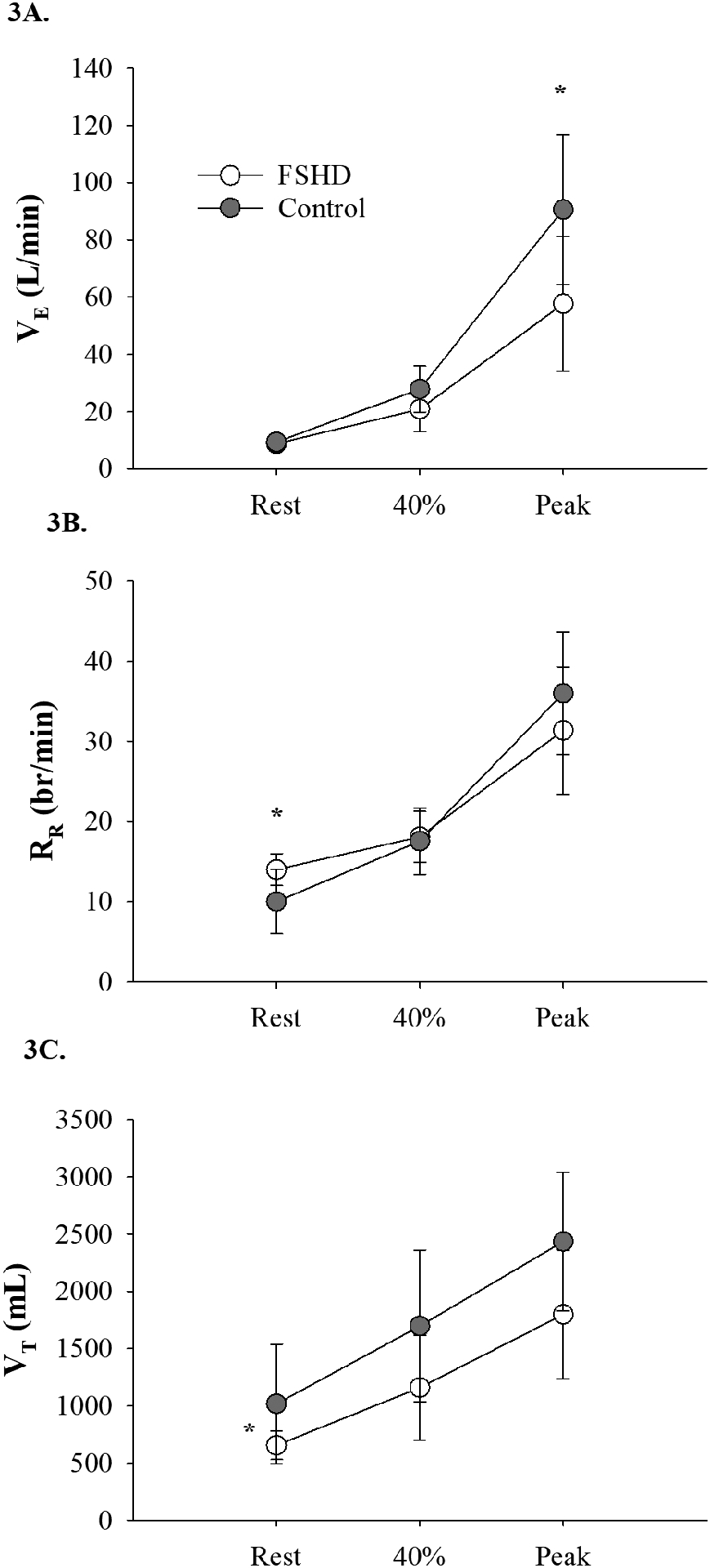
Methods: Eleven people with FSHD (47 ± 13 yr, 4 females) and 11 controls (46 ± 13 yr, 4 females) completed one visit, which included a volitional peak oxygen consumption (V̇O2peak) cycling test. Breath-by-breath gas exchange, ventilation, and cardiovascular responses were measured at rest and during exercise. The test featured 3-min stages (speed, 65-70 rpm) with incremental increases in intensity (FSHD: 20 W per stage; control: 40-60 W per stage). Body lean mass (LM (kg, %)) was collected via dual-energy x-ray absorptiometry.
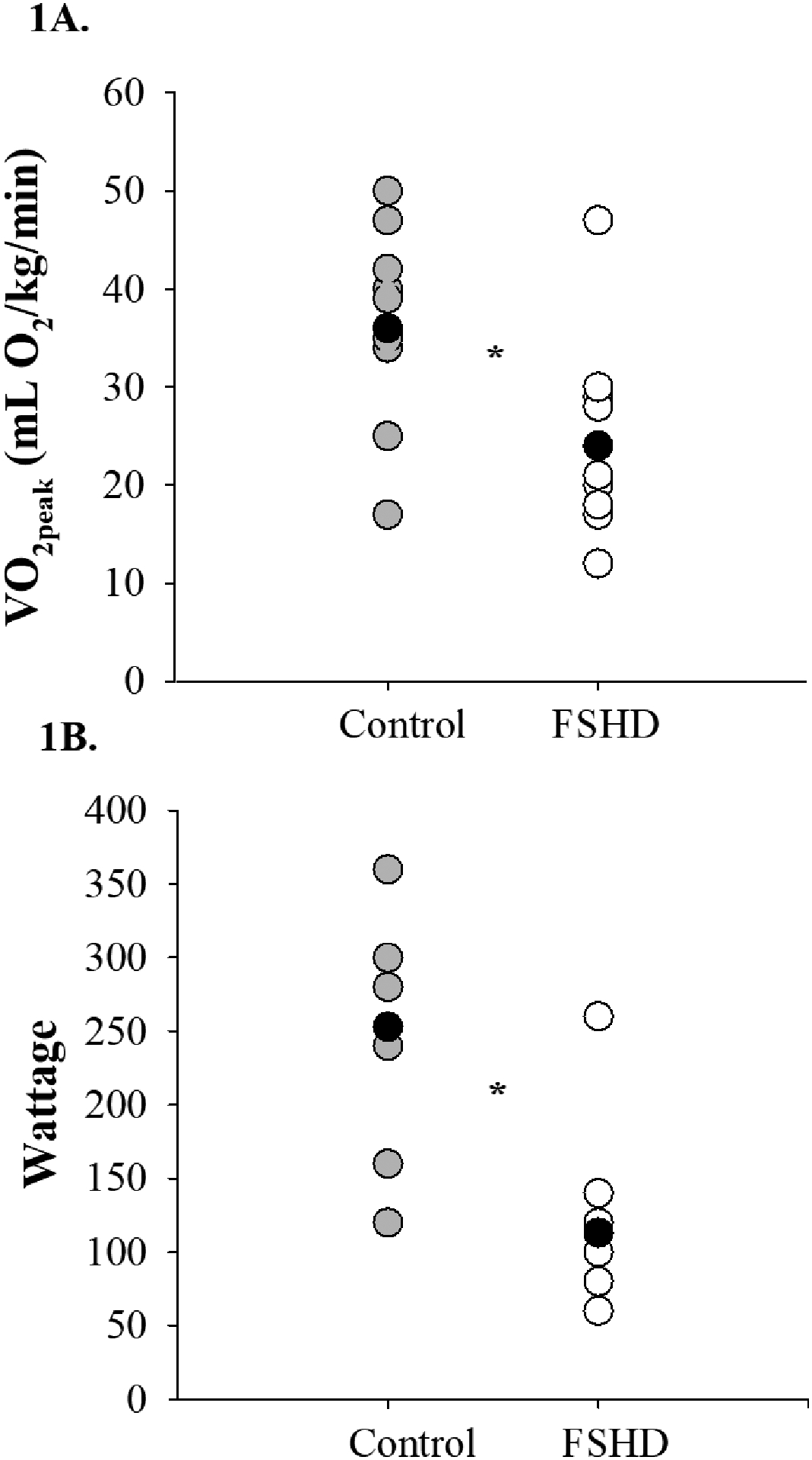
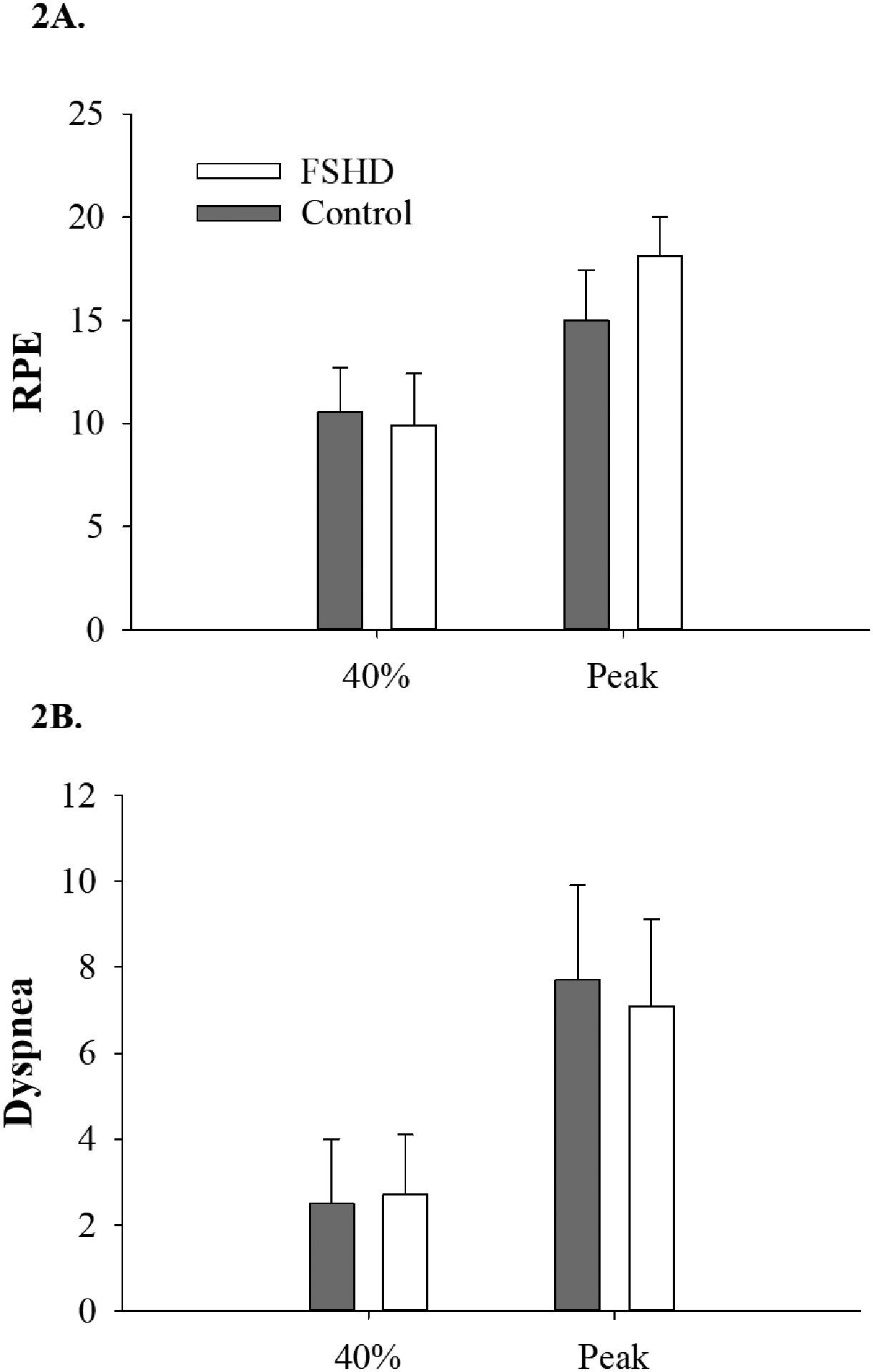
Results: V̇O2peak was 32% lower (24.5 ± 9.7 vs 36.2 ± 9.3 mL·kg-1·min-1, P < 0.01), and wattage was 55% lower in FSHD (112.7 ± 56.1 vs 252.7 ± 67.7 W, P < 0.01). When working at a relative submaximal intensity (40% of V̇O2peak), wattage was 55% lower in FSHD (41.8 ± 30.3 vs 92.7 ± 32.6 W, P = 0.01), although ratings of perceived exertion (FSHD: 11 ± 2 vs control: 10 ± 3, P = 0.61) and dyspnea (FSHD: 3 ± 1 vs control: 3 ± 2, P = 0.78) were similar between groups. At an absolute intensity (60 W), the rating of perceived exertion was 63% higher (13 ± 3 vs 8 ± 2, P < 0.01) and dyspnea was 180% higher in FSHD (4 ± 2 vs 2 ± 2, P < 0.01). V̇O2peak was most strongly correlated with resting O2 pulse in controls (P < 0.01, r = 0.90) and percent leg LM in FSHD (P < 0.01, r = 0.88). Among FSHD participants, V̇O2peak was associated with self-reported functionality (FSHD-HI score; activity limitation: P < 0.01, r = -0.78), indicating a strong association between perceived and objective impairments.
Conclusions: Disease-driven losses of LM contribute to exercise intolerance in FSHD, as evidenced by a lower V̇O2peak and elevated symptoms of dyspnea and fatigue during submaximal exercise. Regular exercise participation may preserve LM, thus providing some protection against exercise tolerance in FSHD.
Copyright © 2022 by the American College of Sports Medicine.
Conflict of interest statement
Conflicts of interest
The authors of this research have no disclosures or competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
