

A polygenic risk score improves risk stratification of coronary artery disease: a large-scale prospective Chinese cohort study
- PMID: 35195259
- PMCID: PMC9076396
- DOI: 10.1093/eurheartj/ehac093
A polygenic risk score improves risk stratification of coronary artery disease: a large-scale prospective Chinese cohort study
Abstract
Aims: To construct a polygenic risk score (PRS) for coronary artery disease (CAD) and comprehensively evaluate its potential in clinical utility for primary prevention in Chinese populations.
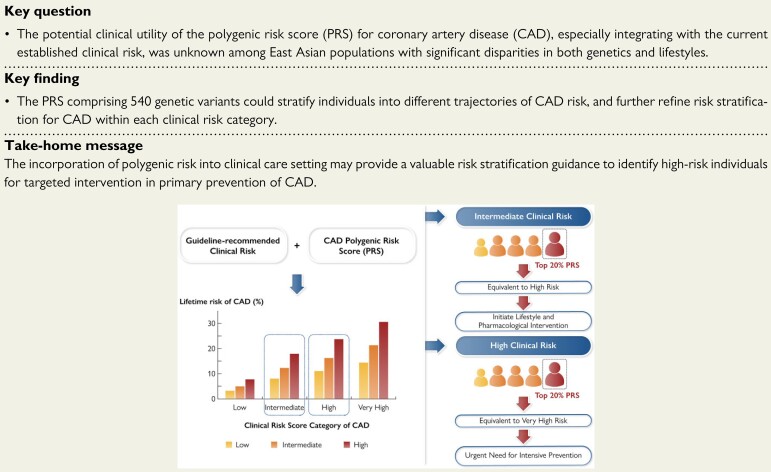
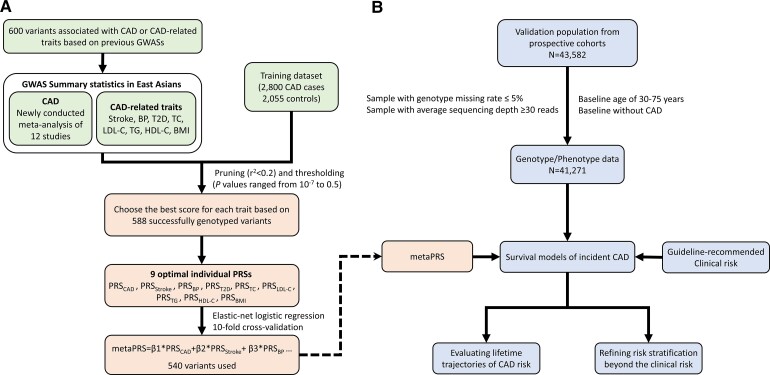
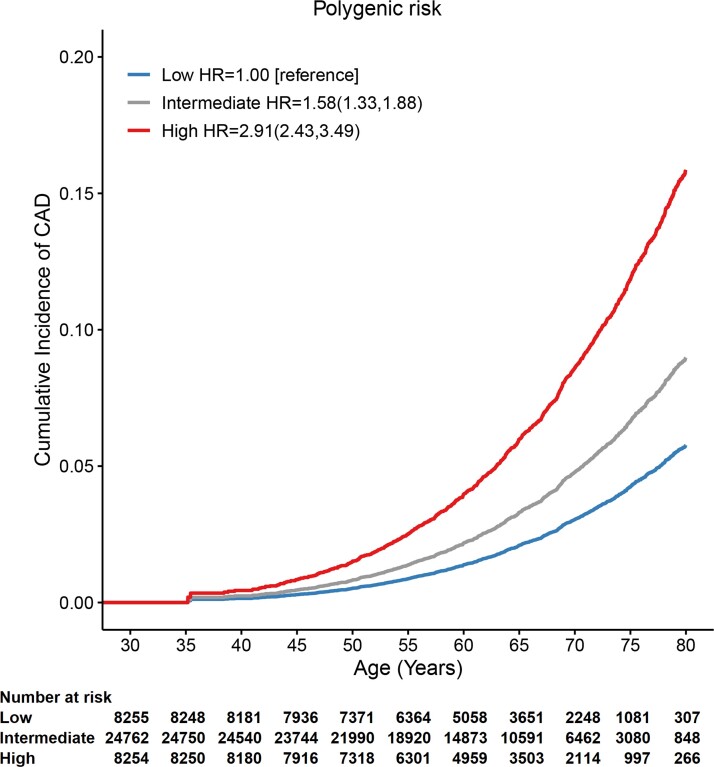
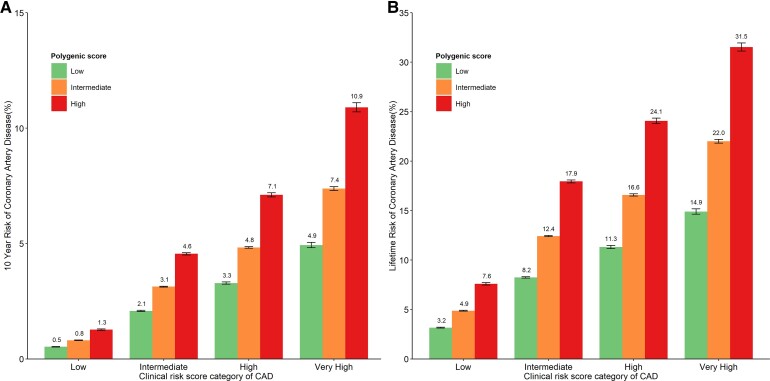
Methods and results: Using meta-analytic approach and large genome-wide association results for CAD and CAD-related traits in East Asians, a PRS comprising 540 genetic variants was developed in a training set of 2800 patients with CAD and 2055 controls, and was further assessed for risk stratification for CAD integrating with the guideline-recommended clinical risk score in large prospective cohorts comprising 41 271 individuals. During a mean follow-up of 13.0 years, 1303 incident CAD cases were identified. Individuals with high PRS (the highest 20%) had about three-fold higher risk of CAD than the lowest 20% (hazard ratio 2.91, 95% confidence interval 2.43-3.49), with the lifetime risk of 15.9 and 5.8%, respectively. The addition of PRS to the clinical risk score yielded a modest yet significant improvement in C-statistic (1%) and net reclassification improvement (3.5%). We observed significant gradients in both 10-year and lifetime risk of CAD according to the PRS within each clinical risk strata. Particularly, when integrating high PRS, intermediate clinical risk individuals with uncertain clinical decision for intervention would reach the risk levels (10-year of 4.6 vs. 4.8%, lifetime of 17.9 vs. 16.6%) of high clinical risk individuals with intermediate (20-80%) PRS.
Conclusion: The PRS could stratify individuals into different trajectories of CAD risk, and further refine risk stratification for CAD within each clinical risk strata, demonstrating a great potential to identify high-risk individuals for targeted intervention in clinical utility.
Keywords: Clinical risk score; Coronary artery disease; Polygenic risk score.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Figures
Comment in
-
Polygenic risk score: a tool ready for clinical use?Eur Heart J. 2022 May 7;43(18):1712-1714. doi: 10.1093/eurheartj/ehab923. Eur Heart J. 2022. PMID: 35211747 No abstract available.
-
The risk of 'hidden' sodium and of low vitamin D levels.Eur Heart J. 2022 May 7;43(18):1687-1690. doi: 10.1093/eurheartj/ehac203. Eur Heart J. 2022. PMID: 35523427 No abstract available.
References
-
- Wang H, Naghavi M, Allen C, Barber RM, Bhutta ZA, Carter A, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1459–1544. - PMC - PubMed
-
- National Center for Cardiovascular Diseases . Report on cardiovascular diseases in China 2019 [Chinese] (Encyclopedia of China Publishing House, 2019).
-
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019;140:e596–e646. - PMC - PubMed
-
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 2020;41:407–477. - PubMed
-
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Back M, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J 2021;42:3227–3337. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
