

Breast cancer screening in sub-Saharan Africa: a systematic review and ethical appraisal
- PMID: 35197002
- PMCID: PMC8867875
- DOI: 10.1186/s12885-022-09299-5
Breast cancer screening in sub-Saharan Africa: a systematic review and ethical appraisal
Erratum in
-
Correction: Breast cancer screening in sub-Saharan Africa: a systematic review and ethical appraisal.BMC Cancer. 2022 Mar 22;22(1):306. doi: 10.1186/s12885-022-09412-8. BMC Cancer. 2022. PMID: 35317782 Free PMC article. No abstract available.
Abstract
Background: The aim of this systematic review was to evaluate the evidence and clinical outcomes of screening interventions and implementation trials in sub-Saharan Africa (SSA) and also appraise some ethical issues related to screening in the region through quantitative and qualitative narrative synthesis of the literature.
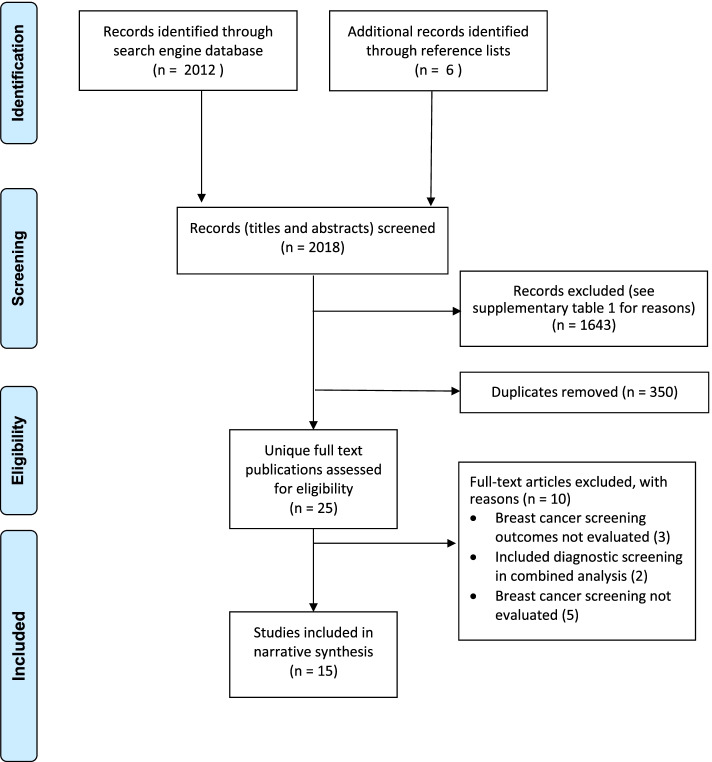
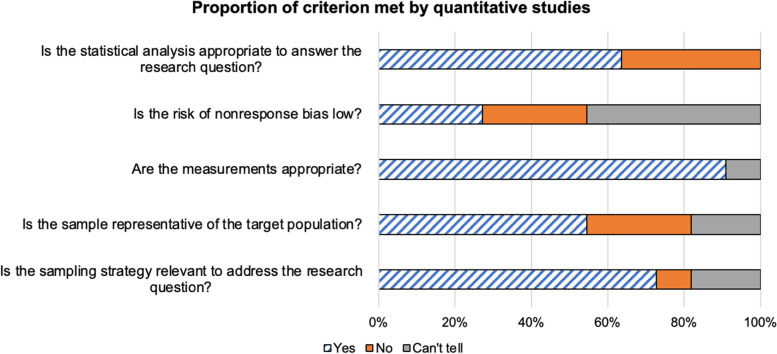
Methods: We searched Pubmed, OvidMEDLINE, Embase, and Web of Science to identify studies published on breast cancer screening interventions and outcomes in SSA. Descriptive statistics were used to summarize the frequency and proportions of extracted variables, and narrative syntheses was used to evaluate the clinical outcomes of the different screening modalities. The mixed methods appraisal tool was used to assess the quality of studies included in the review.
Results: Fifteen studies were included, which consisted of 72,572 women in ten countries in SSA. 63% (8/15) of the included publications evaluated Clinical Breast Examination (CBE), 47% (7/15) evaluated mammography and 7% (1/15) evaluated ultrasound screening. The cancer detection rate was < 1/1000 to 3.3/1000 and 3.3/100 to 56/1000 for CBE and mammography screening respectively. There was a lot of heterogeneity in CBE methods, target age for screening and no clear documentation of screening interval. Cost-effective analyses showed that CBE screening linked to comprehensive cancer care is most cost effective. There was limited discussion of the ethics of screening, including the possible harms of screening in the absence of linkage to care. The gap between conducting good screening program and the appropriate follow-up with diagnosis and treatment remains one of the major challenges of screening in SSA.
Discussion: There is insufficient real-world data to support the systematic implementation of national breast cancer screening in SSA. Further research is needed to answer important questions about screening, and national and international partnerships are needed to ensure that appropriate diagnostic and treatment modalities are available to patients who screen positive.
© 2022. The Author(s).
Conflict of interest statement
The authors have no financial and non-financial competing interests.
Bege Dauda, PhD, is a post-doctoral fellow in the Medical Ethics Division at the University of Pennsylvania in Philadelphia. His academic focus is on ethico-legal challenges and opportunities of benefit sharing in genomic research in Africa, focusing on the H3 Africa initiative. He also has an interest in the ethics of sample sharing and transfer as well as capacity building in research in Low- and Middle-Income Countries.
Verna Vanderpuye, MD, is a radiation and medical oncology physician with over 20 years of experience in treating cancer patients, training young physicians, nurses and other allied health workers and research into cancer in Africa. She has served on committees which influence care and research including the World Health Organization, American Society of Clinical Oncology, European Society of Clinical Oncology and the African Organization for Research and Treatment in Cancer. Dr. Vanderpuye works to improve delivery of academic content to African practitioners and researchers on the continent and is helping to move forward the agenda of implementation research.
Figures
Similar articles
-
Improving early detection of breast cancer in sub-Saharan Africa: why mammography may not be the way forward.Global Health. 2019 Jan 8;15(1):3. doi: 10.1186/s12992-018-0446-6. Global Health. 2019. PMID: 30621753 Free PMC article. Review.
-
A model to enhance breast cancer screening among rural women aged 40-75 years in Sub-Saharan Africa (SSA): A scoping review.J Med Imaging Radiat Sci. 2024 Mar;55(1):109-124. doi: 10.1016/j.jmir.2023.12.003. Epub 2023 Dec 30. J Med Imaging Radiat Sci. 2024. PMID: 38161135
-
Enablers and barriers to the implementation of breast self-examination (BSE) education programmes among adolescent girls in Sub-Saharan Africa (SSA): an integrative systematic review protocol.BMJ Open. 2024 Nov 19;14(11):e078339. doi: 10.1136/bmjopen-2023-078339. BMJ Open. 2024. PMID: 39566941 Free PMC article.
-
Interventions to increase uptake of cervical screening in sub-Saharan Africa: a scoping review using the integrated behavioral model.BMC Public Health. 2020 May 11;20(1):654. doi: 10.1186/s12889-020-08777-4. BMC Public Health. 2020. PMID: 32393218 Free PMC article.
-
Clinical breast examination screening by trained laywomen in Malawi integrated with other health services.J Surg Res. 2016 Jul;204(1):61-7. doi: 10.1016/j.jss.2016.04.017. Epub 2016 Apr 22. J Surg Res. 2016. PMID: 27451869 Free PMC article. Clinical Trial.
Cited by
-
Factors Determining Women's Attitudes and Knowledge Toward Breast Cancer Screening: A Systematic Review.Healthcare (Basel). 2025 Jul 4;13(13):1605. doi: 10.3390/healthcare13131605. Healthcare (Basel). 2025. PMID: 40648630 Free PMC article. Review.
-
Prevalence of presumptive clinical signs of breast cancer among women attending an early detection campaign in Lomé in 2023.Pan Afr Med J. 2025 Apr 9;50:98. doi: 10.11604/pamj.2025.50.98.43237. eCollection 2025. Pan Afr Med J. 2025. PMID: 40607266 Free PMC article.
-
Global patterns and trends in breast cancer incidence and mortality across 185 countries.Nat Med. 2025 Apr;31(4):1154-1162. doi: 10.1038/s41591-025-03502-3. Epub 2025 Feb 24. Nat Med. 2025. PMID: 39994475
-
Global burden and attributable risk factors of breast cancer in young women: historical trends from 1990 to 2019 and forecasts to 2030 by sociodemographic index regions and countries.J Glob Health. 2024 Jul 19;14:04142. doi: 10.7189/jogh.14.04142. J Glob Health. 2024. PMID: 39026460 Free PMC article.
-
Factors influencing clinical breast cancer screening: A cross-sectional study among Islamic women in Kumasi Metropolis of Ghana.PLoS One. 2025 May 23;20(5):e0320726. doi: 10.1371/journal.pone.0320726. eCollection 2025. PLoS One. 2025. PMID: 40408633 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
