

Inflamed and non-inflamed classes of HCC: a revised immunogenomic classification
- PMID: 35197323
- PMCID: PMC9395551
- DOI: 10.1136/gutjnl-2021-325918
Inflamed and non-inflamed classes of HCC: a revised immunogenomic classification
Abstract
Objective: We previously reported a characterisation of the hepatocellular carcinoma (HCC) immune contexture and described an immune-specific class. We now aim to further delineate the immunogenomic classification of HCC to incorporate features that explain responses/resistance to immunotherapy.
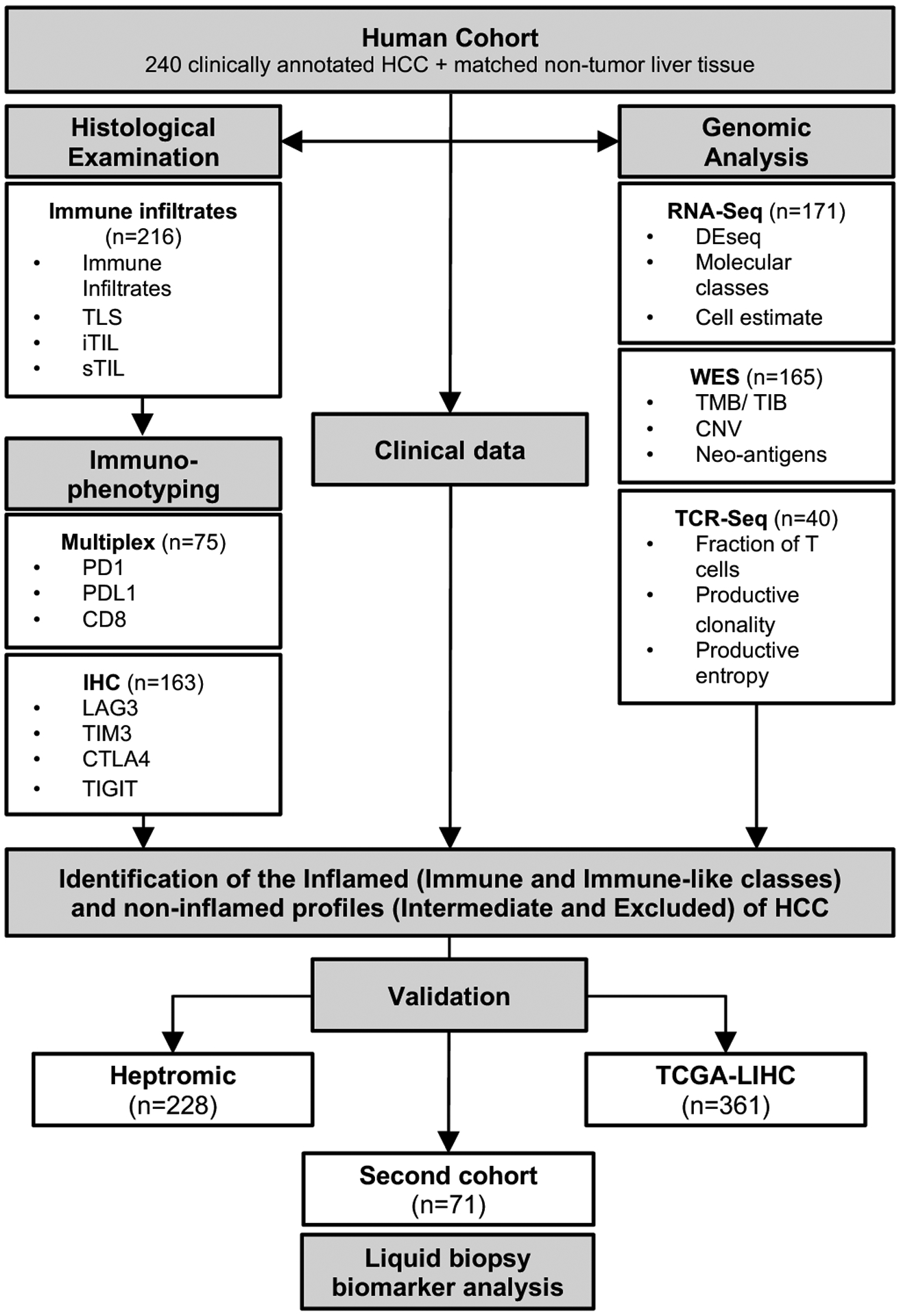
Design: We performed RNA and whole-exome sequencing, T-cell receptor (TCR)-sequencing, multiplex immunofluorescence and immunohistochemistry in a novel cohort of 240 HCC patients and validated our results in other cohorts comprising 660 patients.
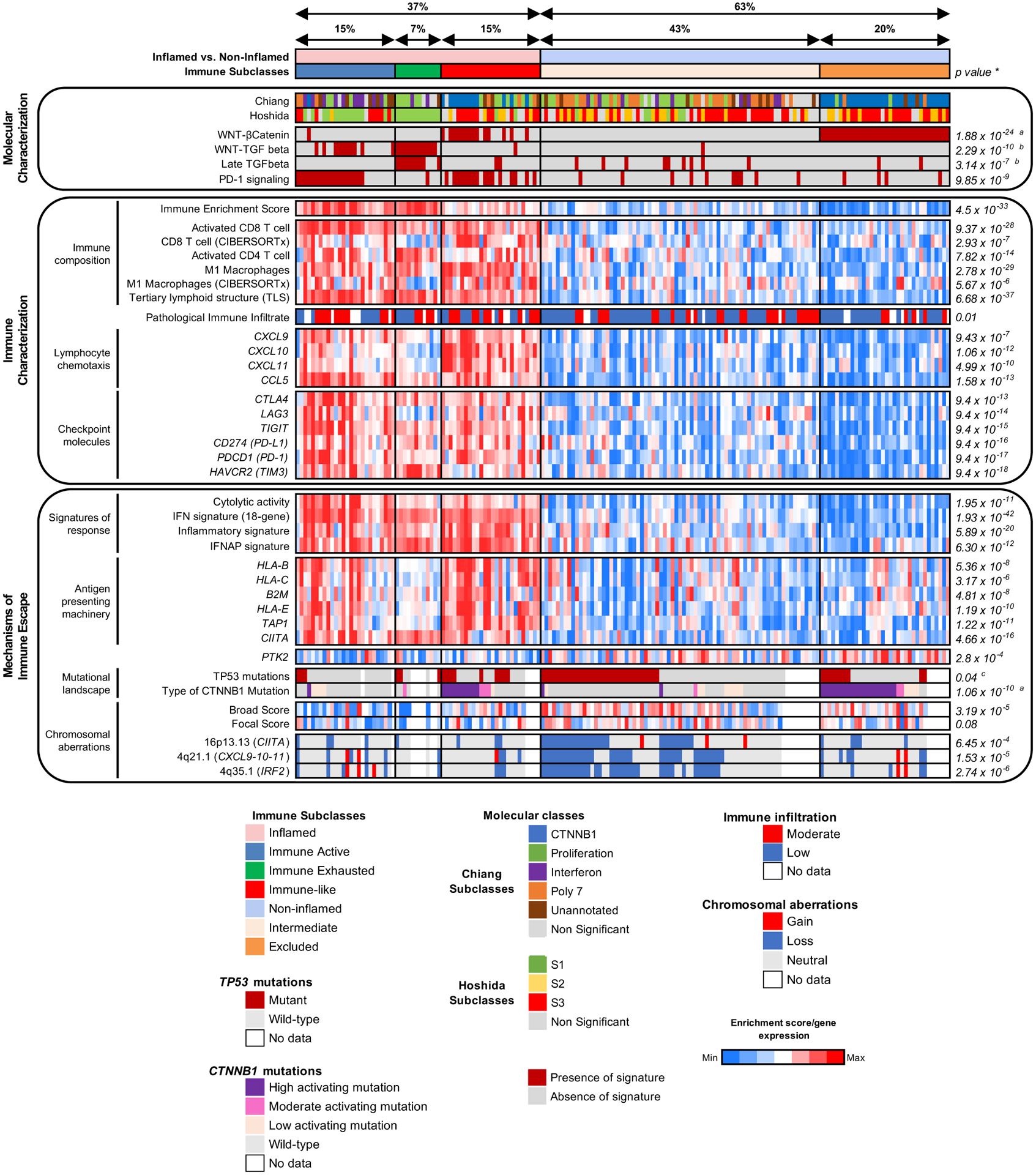
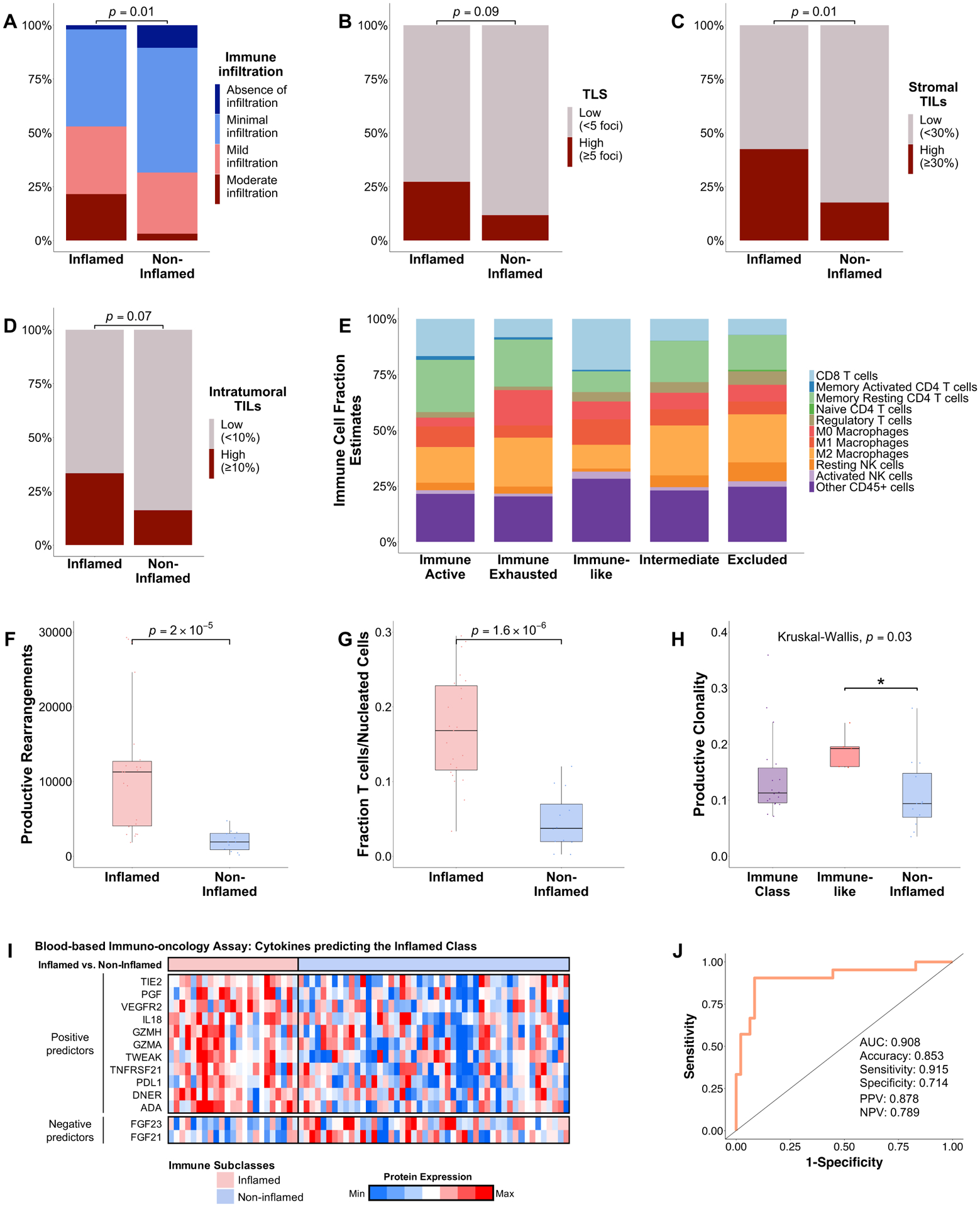
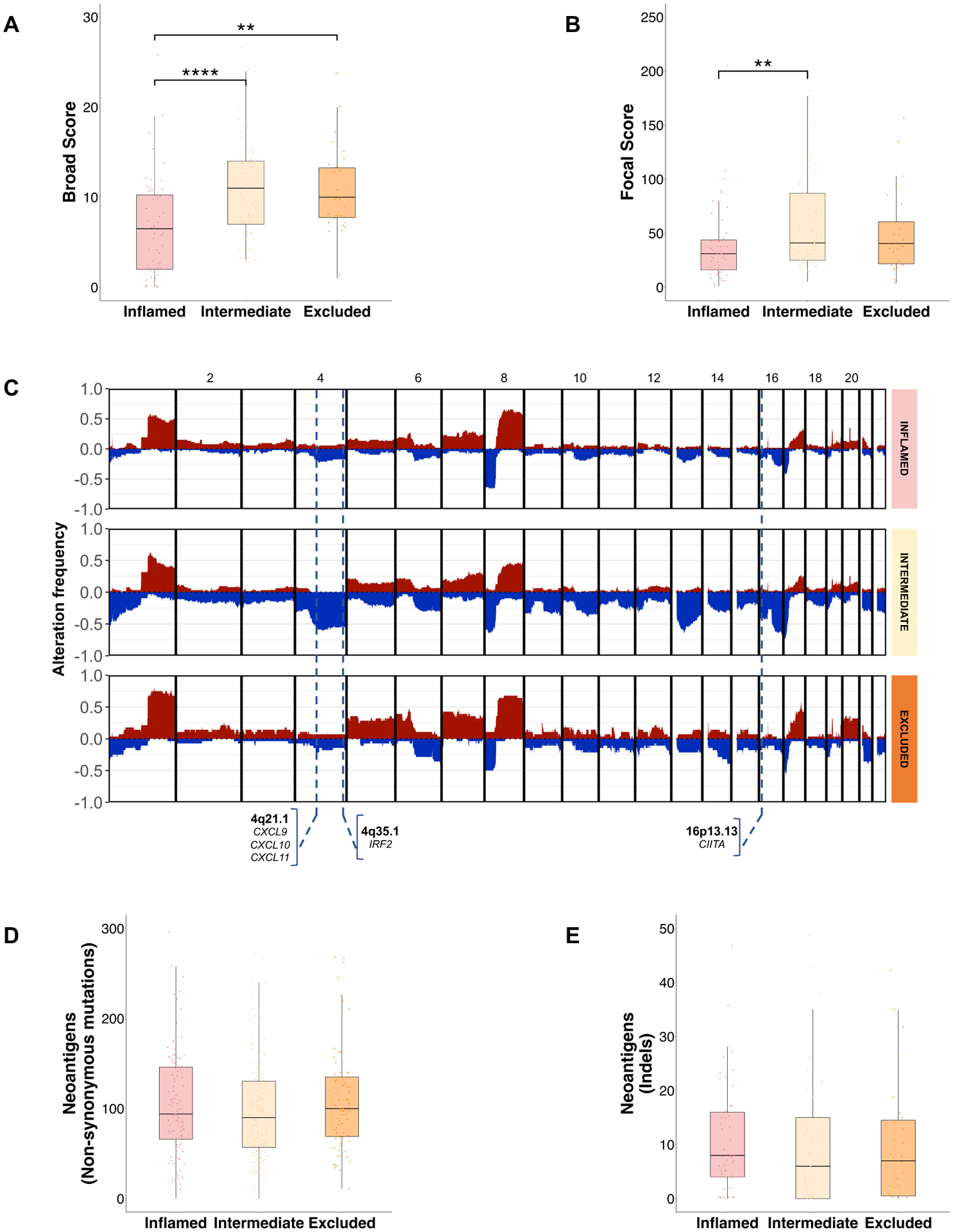
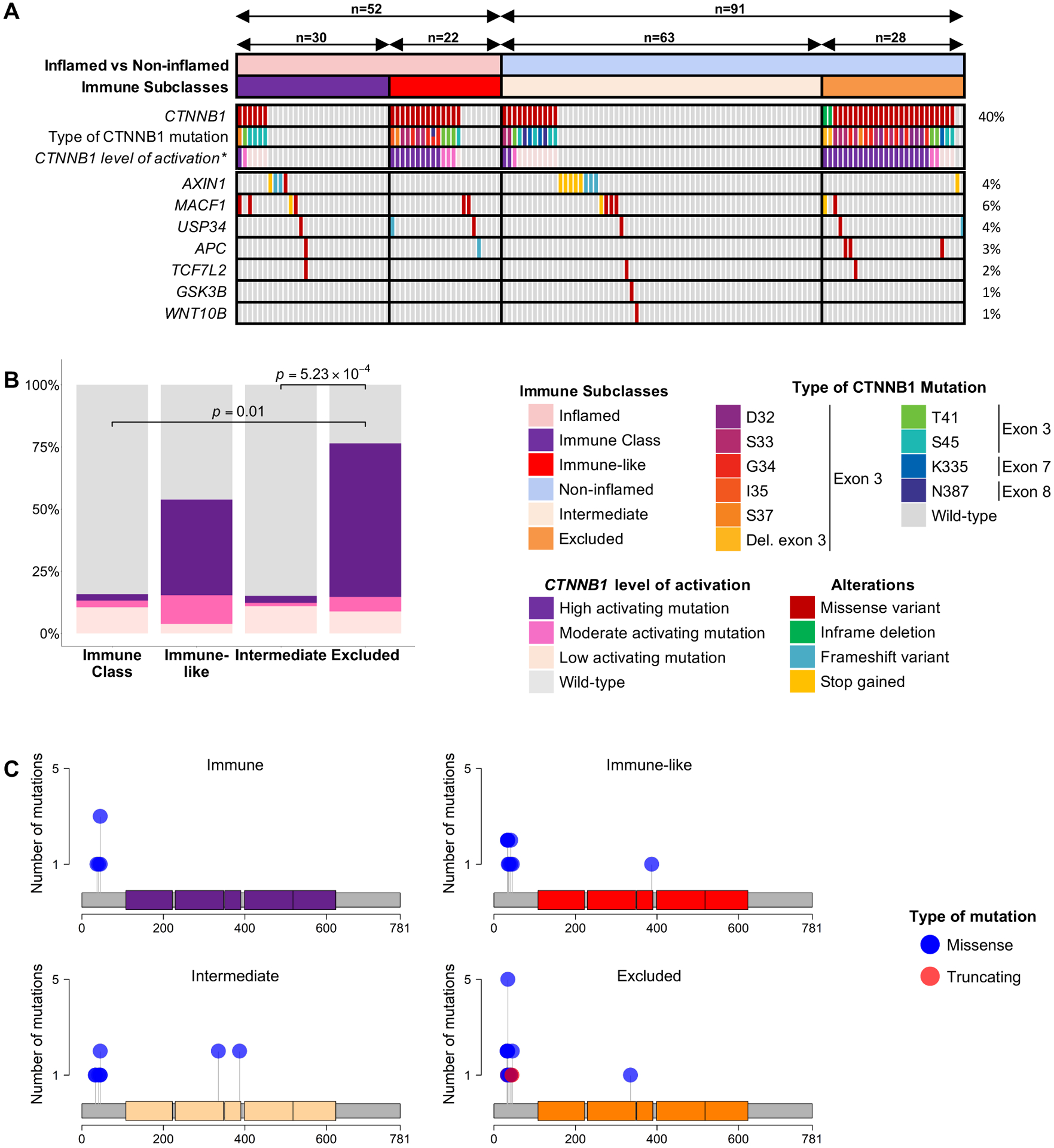
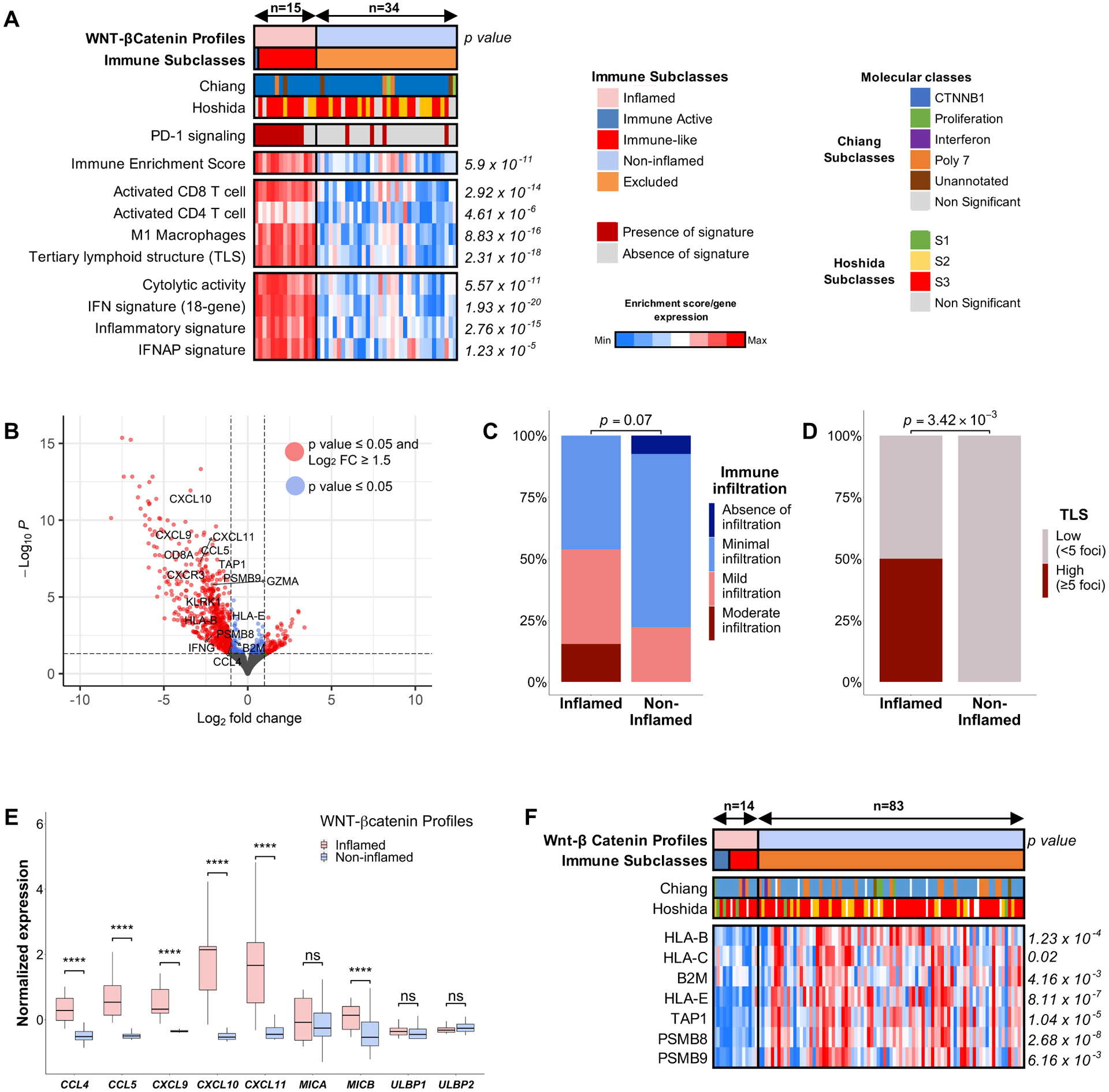
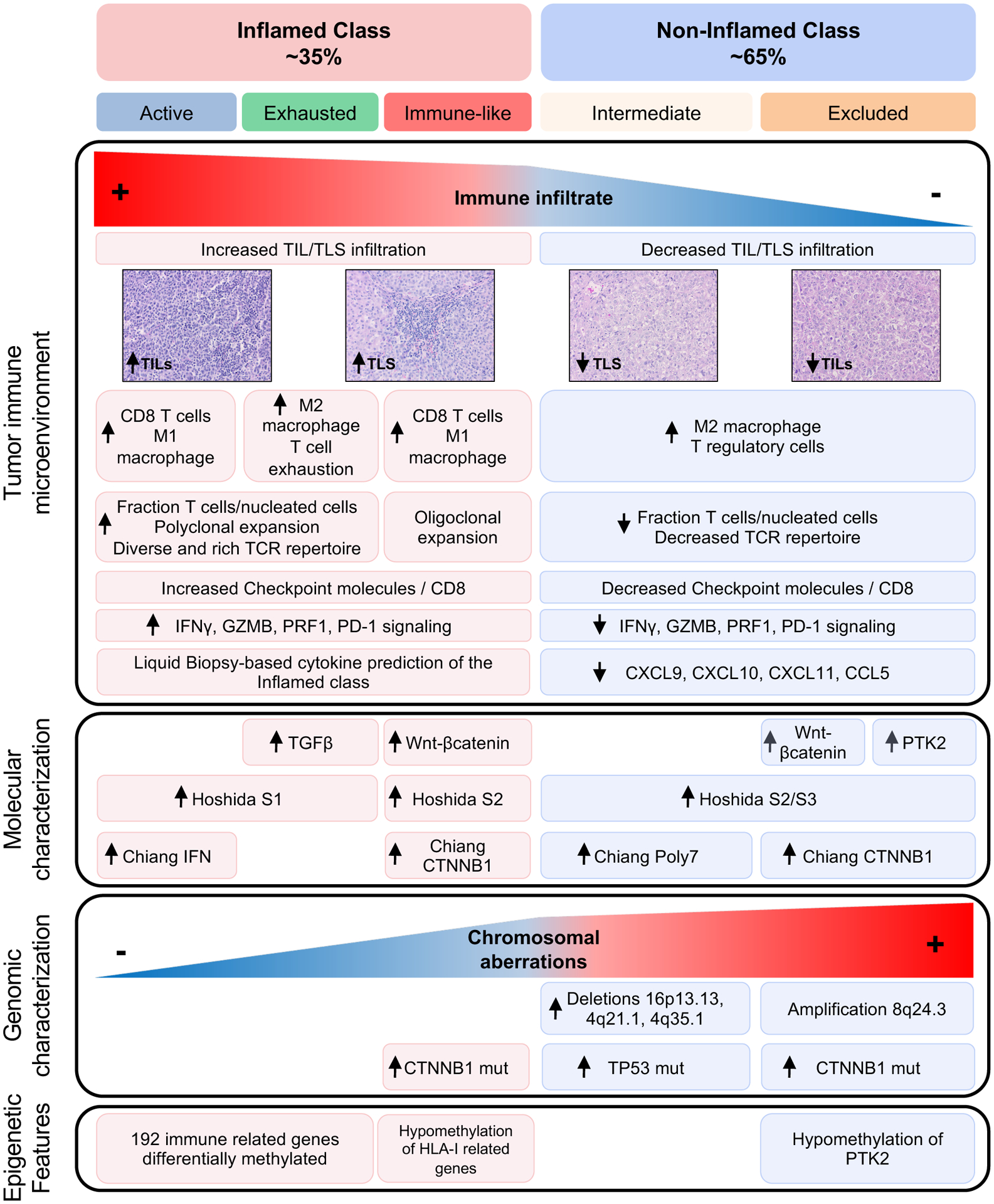
Results: Our integrative analysis led to define: (1) the inflamed class of HCC (37%), which includes the previously reported immune subclass (22%) and a new immune-like subclass (15%) with high interferon signalling, cytolytic activity, expression of immune-effector cytokines and a more diverse T-cell repertoire. A 20-gene signature was able to capture ~90% of these tumours and is associated with response to immunotherapy. Proteins identified in liquid biopsies recapitulated the inflamed class with an area under the ROC curve (AUC) of 0.91; (2) The intermediate class, enriched in TP53 mutations (49% vs 29%, p=0.035), and chromosomal losses involving immune-related genes and; (3) the excluded class, enriched in CTNNB1 mutations (93% vs 27%, p<0.001) and PTK2 overexpression due to gene amplification and promoter hypomethylation. CTNNB1 mutations outside the excluded class led to weak activation of the Wnt-βcatenin pathway or occurred in HCCs dominated by high interferon signalling and type I antigen presenting genes.
Conclusion: We have characterised the immunogenomic contexture of HCC and defined inflamed and non-inflamed tumours. Two distinct CTNNB1 patterns associated with a differential role in immune evasion are described. These features may help predict immune response in HCC.
Keywords: hepatocellular carcinoma; immune response; immunotherapy; liver immunology; molecular oncology.
© Author(s) (or their employer(s)) 2023. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JA and JN are staff scientists from Bristol-Myers Squibb. JML is receiving research support from Bayer HealthCare Pharmaceuticals, Eisai Inc, Bristol-Myers Squibb, Boehringer-Ingelheim and Ipsen, and consulting fees from Eli Lilly, Bayer HealthCare Pharmaceuticals, Bristol-Myers Squibb, Eisai Inc, Celsion Corporation, Exelixis, Merck, Ipsen, Genentech, Roche, Glycotest, Nucleix, Sirtex, Mina Alpha Ltd and AstraZeneca. The remaining coauthors have nothing to disclose related to this manuscript.
Figures
Comment in
-
Immunogenomic classification of hepatocellular carcinoma patients for immune check-point inhibitors therapy: cui bono?Gut. 2023 Jan;72(1):7-9. doi: 10.1136/gutjnl-2022-327132. Epub 2022 Apr 26. Gut. 2023. PMID: 35474266 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous