

Analysis of eGFR index category and annual eGFR slope association with adverse clinical outcomes using real-world Japanese data: a retrospective database study
- PMID: 35197338
- PMCID: PMC8867325
- DOI: 10.1136/bmjopen-2021-052246
Analysis of eGFR index category and annual eGFR slope association with adverse clinical outcomes using real-world Japanese data: a retrospective database study
Abstract
Objectives: Real-world clinical outcome data of patients with an above-normal estimated glomerular filtration rate (eGFR) and increasing eGFR over time (eGFR slope) are scarce. Although eGFR is commonly recorded, eGFR slopes are rarely used for adverse outcome risk categorisation in clinical practice. We investigated the association of above-normal/below-normal eGFR ranges and increasing/declining eGFR slopes with clinical outcomes in Japan.
Design: Observational cohort study.
Setting: Primary and acute care hospitals; 423 centres.
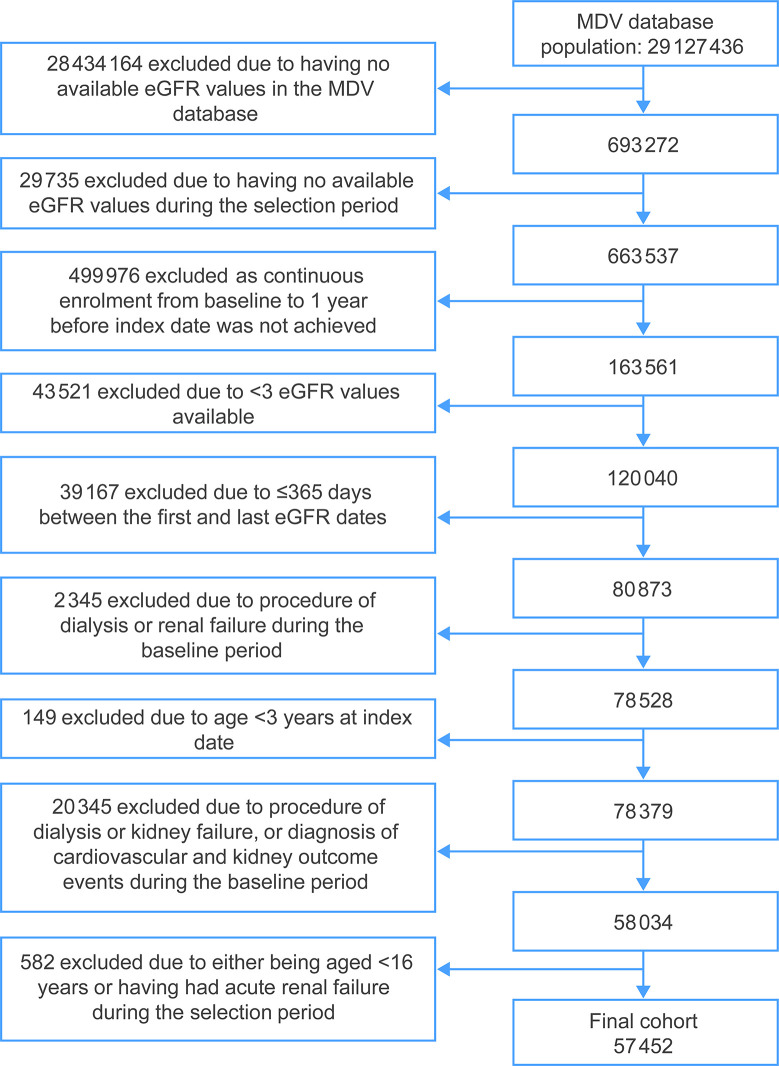
Participants: 57 452 patients aged ≥16 years with ≥3 eGFR values (latest available January 2013-December 2016) from the Japanese Medical Data Vision database were stratified into six index eGFR and six eGFR slope groups (slopes calculated using a linear mixed model).
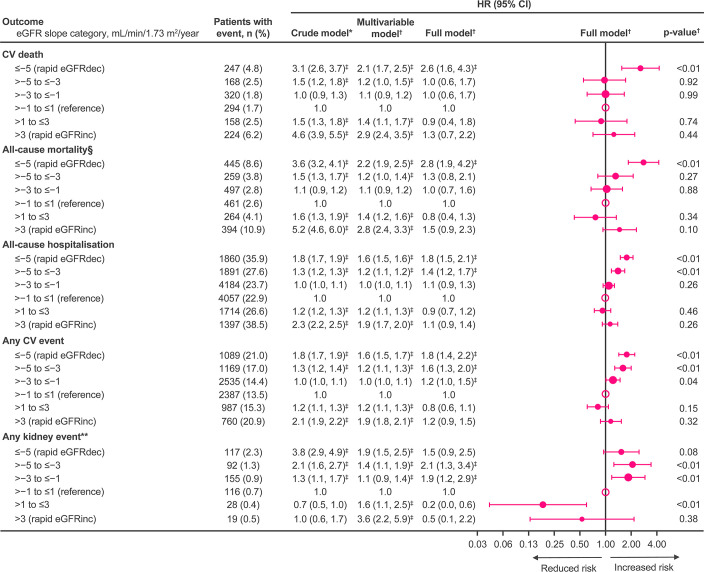
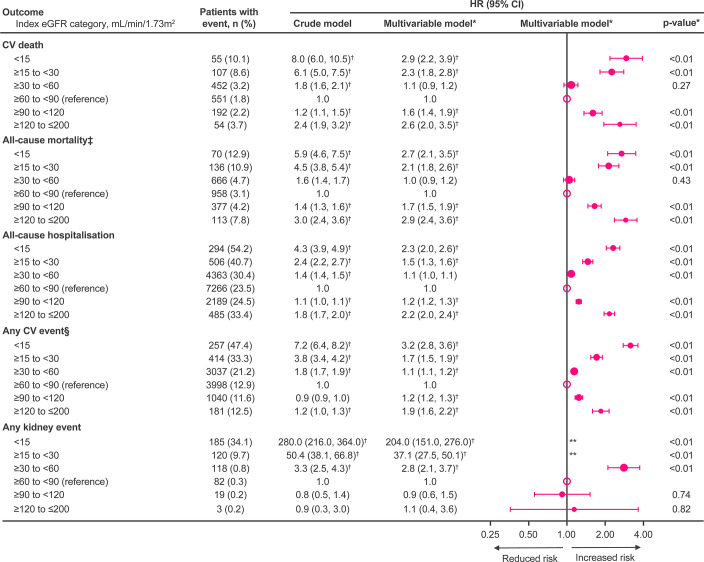
Primary and secondary outcome measures: Time-to-event analyses of cardiovascular mortality, all-cause mortality (ACM), all-cause hospitalisation (ACH) and cardiovascular and major kidney events. eGFR and slope groups were analysed by Cox proportional hazard models with multivariable adjustment, using normal eGFR/little-to-no slope groups as reference.
Results: Higher risk of clinical outcomes was observed with declining eGFR slope groups versus the reference group; the HR (95% CI) for slope ≤-5 mL/min/1.73 m2/year: cardiovascular events 1.8 (1.4 to 2.2), ACH 1.8 (1.5 to 2.1), and ACM 2.8 (1.9 to 4.2) and was non-significant for kidney events 1.5 (0.9 to 2.5). A similar, but non-significant, pattern was observed with increasing slope groups (slope >3 mL/min/1.73 m2/year HR (95% CI): cardiovascular events 1.2 (0.9 to 1.5), ACH 1.1 (0.9 to 1.4) and ACM 1.5 (0.9 to 2.3)).Above-normal and below-normal eGFR groups were associated with poorer outcomes versus the reference group, but kidney events were associated with below-normal eGFR only.
Conclusion: Poorer clinical outcomes were observed not only for below-normal eGFR and declining eGFR slope groups but also for certain above-normal eGFR and increasing slope groups. eGFR and eGFR slope may, therefore, be useful for identifying patients at high risk of adverse clinical outcomes.
Keywords: acute renal failure; cardiology; nephrology; risk management.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: LZ, SH, YO, DS and YN are employees of Boehringer Ingelheim. MHK was an employee of Boehringer Ingelheim at the time of the study. KK received lecture honoraria from Astellas, AstraZeneca, Boehringer Ingelheim, Dainippon-Sumitomo Pharma, Eli Lilly, Kyowa-Hakko Kirin, Mitsubishi-Tanabe, MSD, Novo Nordisk, Ono, Sanofi, and Taisho-Toyama; scholarship grants from Boehringer Ingelheim (Japan), Chugai, Kowa, Mitsubishi-Tanabe, and Ono; and joint research grants from Boehringer Ingelheim (Japan) and Taisho-Toyama. Boehringer Ingelheim (Japan), Kyowa-Hakko Kirin, Mitsubishi-Tanabe, Ono, and Taisho-Toyama contributed to establishing the Division of Anticipatory Molecular Food Science and Technology, Medical Research Institute, Kanazawa Medical University.
Figures
Similar articles
-
Is there a correlation between an eGFR slope measured over a 5-year period and incident cardiovascular events in the following 5 years among a Flemish general practice population: a retrospective cohort study.BMJ Open. 2018 Nov 12;8(11):e023594. doi: 10.1136/bmjopen-2018-023594. BMJ Open. 2018. PMID: 30420350 Free PMC article.
-
The relationship between eGFR slope and subsequent risk of vascular outcomes and all-cause mortality in type 2 diabetes: the ADVANCE-ON study.Diabetologia. 2019 Nov;62(11):1988-1997. doi: 10.1007/s00125-019-4948-4. Epub 2019 Jul 13. Diabetologia. 2019. PMID: 31302707 Free PMC article. Clinical Trial.
-
Slope of Kidney Function and Its Association with Longitudinal Mortality and Cardiovascular Disease among Individuals with CKD.J Am Soc Nephrol. 2020 Dec;31(12):2912-2923. doi: 10.1681/ASN.2020040476. Epub 2020 Oct 6. J Am Soc Nephrol. 2020. PMID: 33023926 Free PMC article.
-
eGFR slope as a surrogate endpoint for clinical study in early stage of chronic kidney disease: from The Japan Chronic Kidney Disease Database.Clin Exp Nephrol. 2023 Oct;27(10):847-856. doi: 10.1007/s10157-023-02376-4. Epub 2023 Jul 19. Clin Exp Nephrol. 2023. PMID: 37466813 Free PMC article.
-
Estimated Glomerular Filtration Rate (eGFR) Slope Assessment as a Surrogate End-point in Cardiovascular trials: Implications, Impediments, and Future Directions.Curr Probl Cardiol. 2023 Mar;48(3):101508. doi: 10.1016/j.cpcardiol.2022.101508. Epub 2022 Nov 17. Curr Probl Cardiol. 2023. PMID: 36402218 Review. No abstract available.
Cited by
-
Patient Management and Clinical Outcomes Associated with a Recorded Diagnosis of Stage 3 Chronic Kidney Disease: The REVEAL-CKD Study.Adv Ther. 2023 Jun;40(6):2869-2885. doi: 10.1007/s12325-023-02482-5. Epub 2023 May 3. Adv Ther. 2023. PMID: 37133647 Free PMC article.
-
Long-Term Effect of Semaglutide on the Glomerular Filtration Rate Slope in High-Risk Patients with Diabetic Nephropathy: Analysis in Real-World Clinical Practice.Pharmaceutics. 2025 Jul 21;17(7):943. doi: 10.3390/pharmaceutics17070943. Pharmaceutics. 2025. PMID: 40733151 Free PMC article.
-
Impaired renal function in patients with permanent hypoparathyroidism after thyroidectomy: analysis of a nationwide cohort in Spain.Endocrine. 2025 Jun;88(3):826-835. doi: 10.1007/s12020-025-04187-x. Epub 2025 Mar 3. Endocrine. 2025. PMID: 40032798
-
Is eGFR Slope a Novel Predictor of Chronic Complications of Type 2 Diabetes Mellitus? A Systematic Review and Meta-Analysis.J Diabetes Res. 2024 Jan 17;2024:8859678. doi: 10.1155/2024/8859678. eCollection 2024. J Diabetes Res. 2024. PMID: 38268787 Free PMC article.
References
-
- Chronic Kidney Disease Prognosis Consortium, Matsushita K, van der Velde M, et al. . Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 2010;375:2073–81. 10.1016/S0140-6736(10)60674-5 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous