

Clinical feasibility of a contactless multiparameter continuous monitoring technology for neonates in a large public maternity hospital in Nairobi, Kenya
- PMID: 35197529
- PMCID: PMC8866488
- DOI: 10.1038/s41598-022-07189-1
Clinical feasibility of a contactless multiparameter continuous monitoring technology for neonates in a large public maternity hospital in Nairobi, Kenya
Abstract
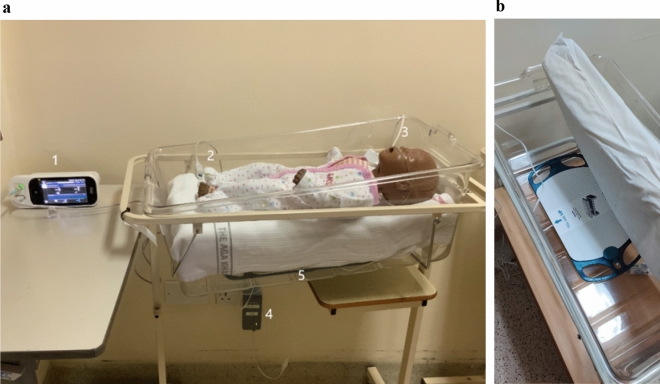
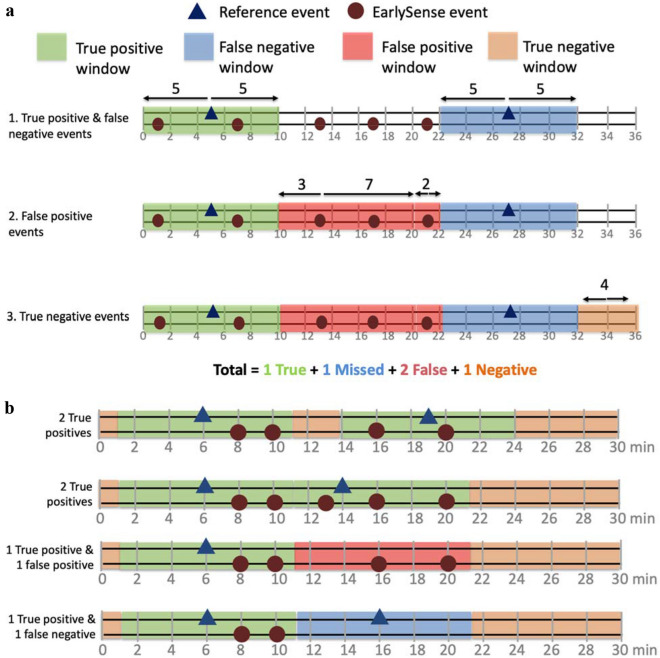
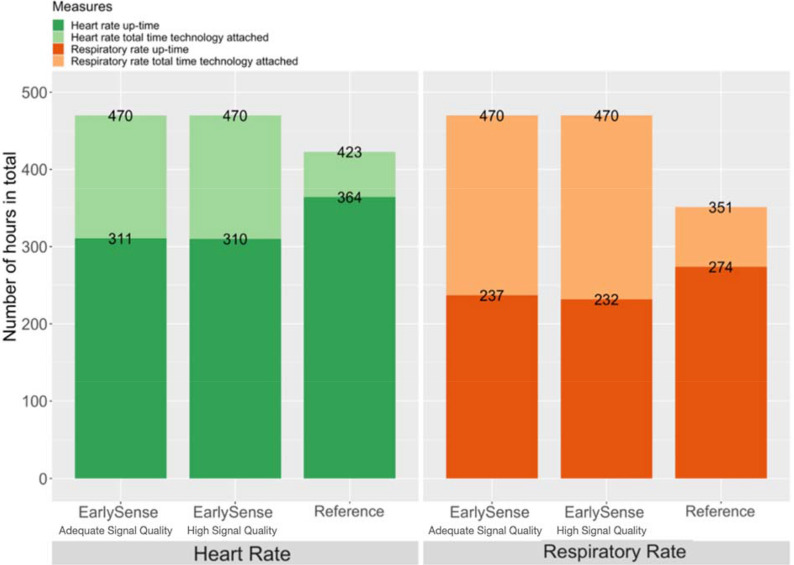
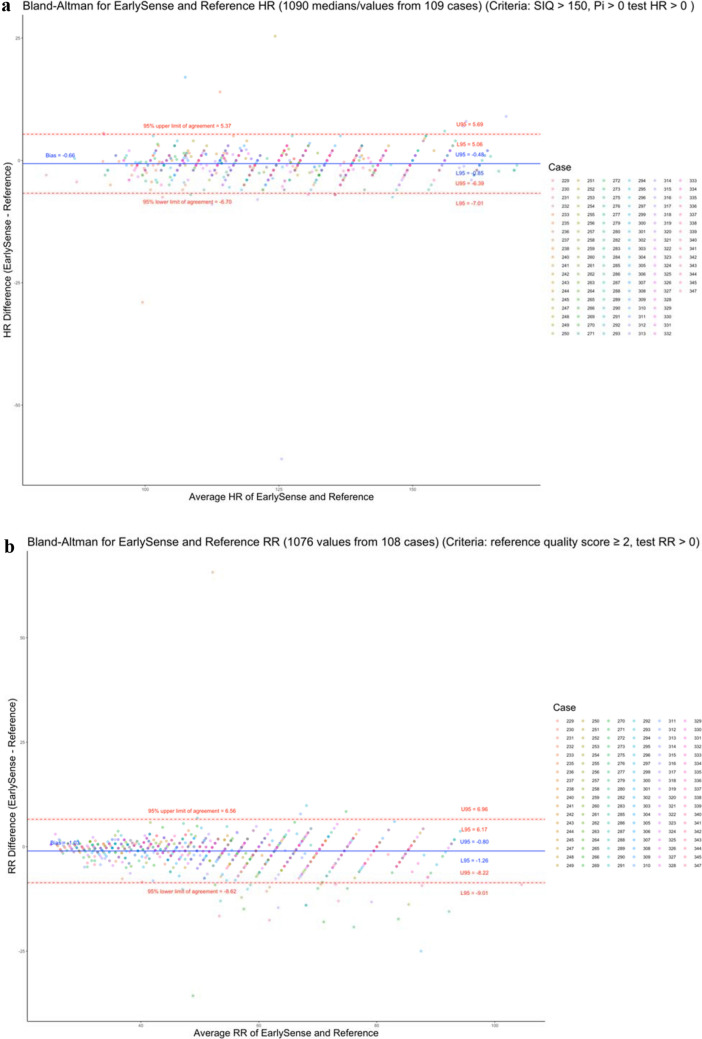
Multiparameter continuous physiological monitoring (MCPM) technologies are critical in the clinical management of high-risk neonates; yet, these technologies are frequently unavailable in many African healthcare facilities. We conducted a prospective clinical feasibility study of EarlySense's novel under-mattress MCPM technology in neonates at Pumwani Maternity Hospital in Nairobi, Kenya. To assess feasibility, we compared the performance of EarlySense's technology to Masimo's Rad-97 pulse CO-oximeter with capnography technology for heart rate (HR) and respiratory rate (RR) measurements using up-time, clinical event detection performance, and accuracy. Between September 15 and December 15, 2020, we collected and analyzed 470 hours of EarlySense data from 109 enrolled neonates. EarlySense's technology's up-time per neonate was 2.9 (range 0.8, 5.3) hours for HR and 2.1 (range 0.9, 4.0) hours for RR. The difference compared to the reference was a median of 0.6 (range 0.1, 3.1) hours for HR and 0.8 (range 0.1, 2.9) hours for RR. EarlySense's technology identified high HR and RR events with high sensitivity (HR 81%; RR 83%) and specificity (HR 99%; RR 83%), but was less sensitive for low HR and RR (HR 0%; RR 14%) although maintained specificity (HR 100%; RR 95%). There was a greater number of false negative and false positive RR events than false negative and false positive HR events. The normalized spread of limits of agreement was 9.6% for HR and 28.6% for RR, which met the a priori-identified limit of 30%. EarlySense's MCPM technology was clinically feasible as demonstrated by high percentage of up-time, strong clinical event detection performance, and agreement of HR and RR measurements compared to the reference technology. Studies in critically ill neonates, assessing barriers and facilitators to adoption, and costing analyses will be key to the technology's development and potential uptake and scale-up.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- United Nations Inter-agency Group for Child Mortality Estimation . Levels & Trends in Child Mortality: Report 2019, Estimates Developed by the United Nations Inter-agency Group for Child Mortality Estimation. United Nations Fund; 2019.
-
- World Health Organization. Newborns: Improving Survival and Well-Being (2020). https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-morta... (Accessed 22 January 2021).
-
- Mitchell EJ, Qureshi ZP, Were F, et al. Feasibility of using an early warning score for preterm or low birthweight infants in a low-resource setting: Results of a mixed-methods study at a national referral hospital in Kenya. BMJ Open. 2020;10(10):e039061. doi: 10.1136/bmjopen-2020-039061. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
