

Integration of questionnaire-based risk factors improves polygenic risk scores for human coronary heart disease and type 2 diabetes
- PMID: 35197564
- PMCID: PMC8866413
- DOI: 10.1038/s42003-021-02996-0
Integration of questionnaire-based risk factors improves polygenic risk scores for human coronary heart disease and type 2 diabetes
Abstract
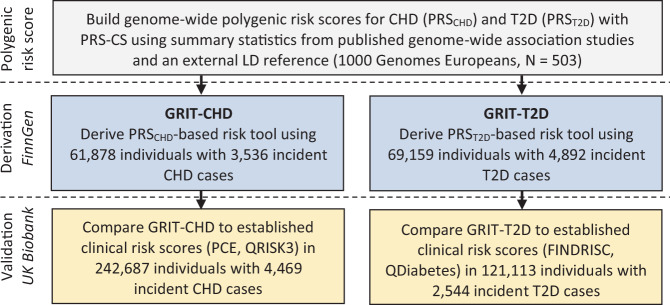
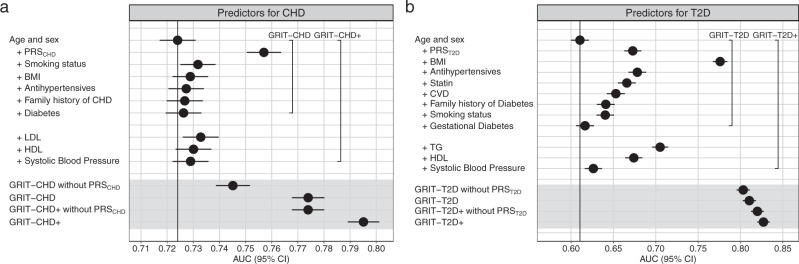
Large-scale biobank initiatives and commercial repositories store genomic data collected from millions of individuals, and tools to leverage the rapidly growing pool of health and genomic data in disease prevention are needed. Here, we describe the derivation and validation of genomics-enhanced risk tools for two common cardiometabolic diseases, coronary heart disease and type 2 diabetes. Data used for our analyses include the FinnGen study (N = 309,154) and the UK Biobank project (N = 343,672). The risk tools integrate contemporary genome-wide polygenic risk scores with simple questionnaire-based risk factors, including demographic, lifestyle, medication, and comorbidity data, enabling risk calculation across resources where genome data is available. Compared to routinely used clinical risk scores for coronary heart disease and type 2 diabetes prevention, the risk tools show at least equivalent risk discrimination, improved risk reclassification (overall net reclassification improvements ranging from 3.7 [95% CI 2.8-4.6] up to 6.2 [4.6-7.8]), and capacity to be improved even further with standard lipid and blood pressure measurements. Without the need for blood tests or evaluation by a health professional, the risk tools provide a powerful yet simple method for preliminary cardiometabolic risk assessment for individuals with genome data available.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
