

Neurological manifestations of long-COVID syndrome: a narrative review
- PMID: 35198136
- PMCID: PMC8859684
- DOI: 10.1177/20406223221076890
Neurological manifestations of long-COVID syndrome: a narrative review
Abstract
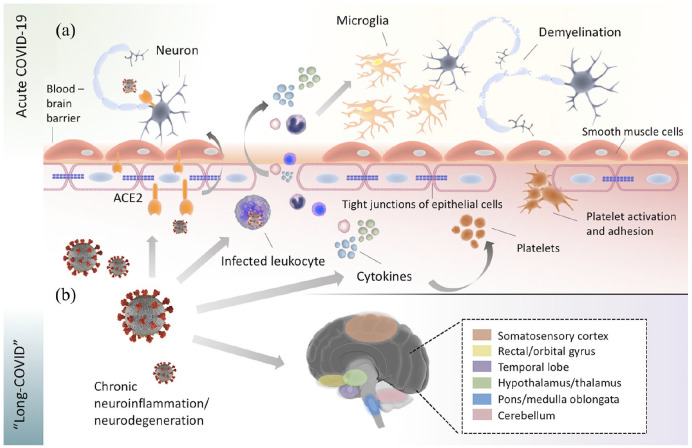
Accumulating evidence points toward a very high prevalence of prolonged neurological symptoms among coronavirus disease 2019 (COVID-19) survivors. To date, there are no solidified criteria for 'long-COVID' diagnosis. Nevertheless, 'long-COVID' is conceptualized as a multi-organ disorder with a wide spectrum of clinical manifestations that may be indicative of underlying pulmonary, cardiovascular, endocrine, hematologic, renal, gastrointestinal, dermatologic, immunological, psychiatric, or neurological disease. Involvement of the central or peripheral nervous system is noted in more than one-third of patients with antecedent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, while an approximately threefold higher incidence of neurological symptoms is recorded in observational studies including patient-reported data. The most frequent neurological manifestations of 'long-COVID' encompass fatigue; 'brain fog'; headache; cognitive impairment; sleep, mood, smell, or taste disorders; myalgias; sensorimotor deficits; and dysautonomia. Although very limited evidence exists to date on the pathophysiological mechanisms implicated in the manifestation of 'long-COVID', neuroinflammatory and oxidative stress processes are thought to prevail in propagating neurological 'long-COVID' sequelae. In this narrative review, we sought to present a comprehensive overview of our current understanding of clinical features, risk factors, and pathophysiological processes of neurological 'long-COVID' sequelae. Moreover, we propose diagnostic and therapeutic algorithms that may aid in the prompt recognition and management of underlying causes of neurological symptoms that persist beyond the resolution of acute COVID-19. Furthermore, as causal treatments for 'long-COVID' are currently unavailable, we propose therapeutic approaches for symptom-oriented management of neurological 'long-COVID' symptoms. In addition, we emphasize that collaborative research initiatives are urgently needed to expedite the development of preventive and therapeutic strategies for neurological 'long-COVID' sequelae.
Keywords: COVID-19; SARS-CoV-2; long-COVID; long-haul; neurological manifestations; post-acute sequelae of SARS-CoV-2.
© The Author(s), 2022.
Conflict of interest statement
Conflict of interest statement: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
