

Urgent Endoscopic Retrograde Cholangiopancreatography (ERCP) vs. Conventional Approach in Acute Biliary Pancreatitis Without Cholangitis: An Updated Systematic Review and Meta-Analysis
- PMID: 35198265
- PMCID: PMC8852244
- DOI: 10.7759/cureus.21342
Urgent Endoscopic Retrograde Cholangiopancreatography (ERCP) vs. Conventional Approach in Acute Biliary Pancreatitis Without Cholangitis: An Updated Systematic Review and Meta-Analysis
Abstract
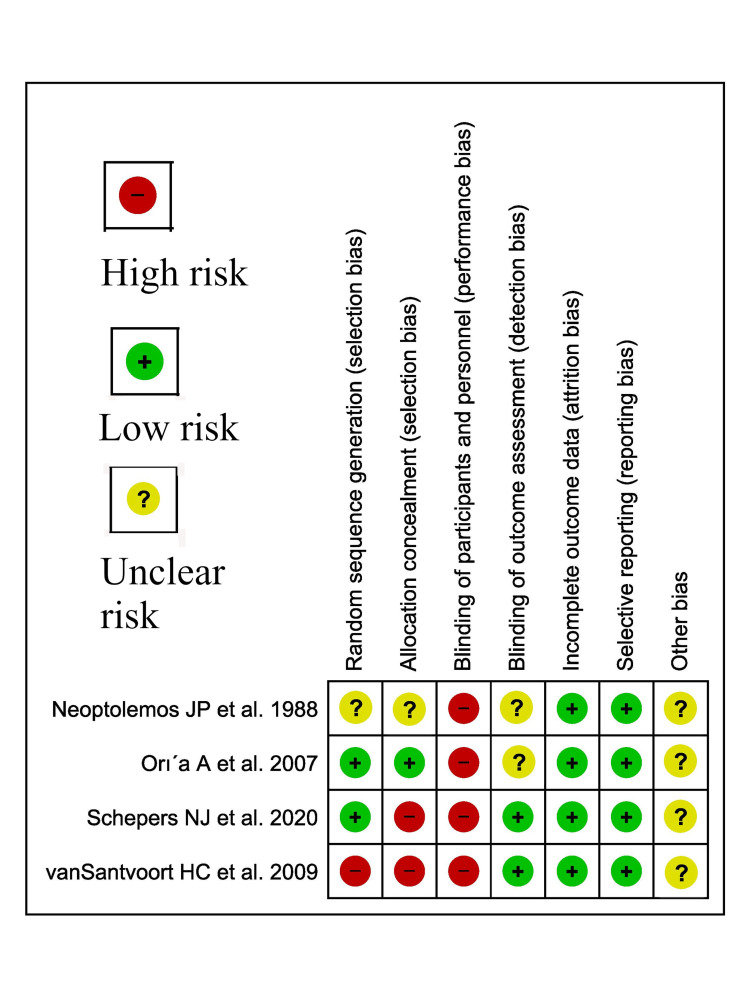
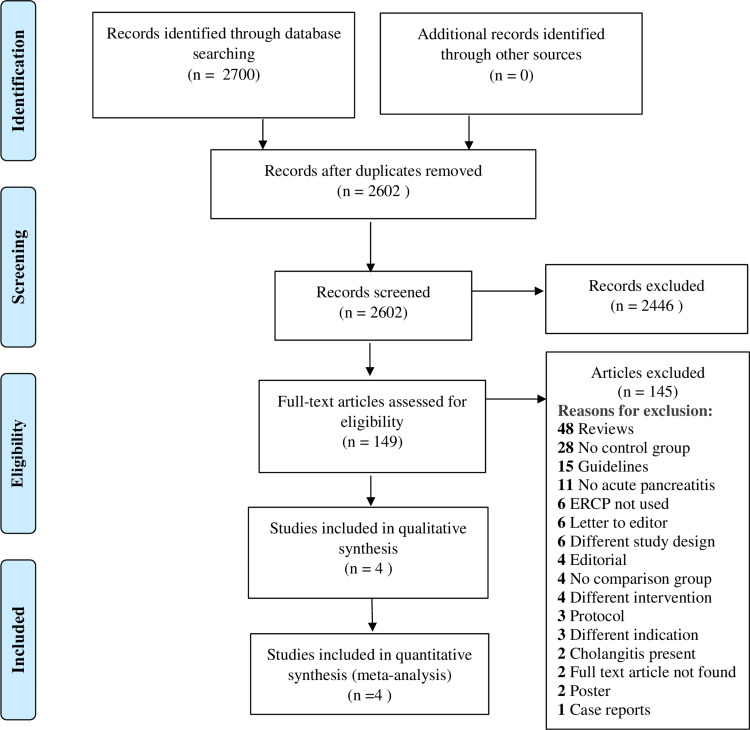
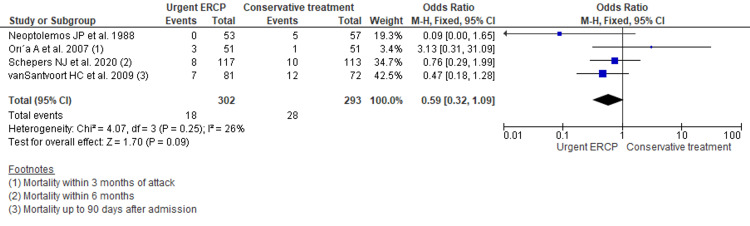
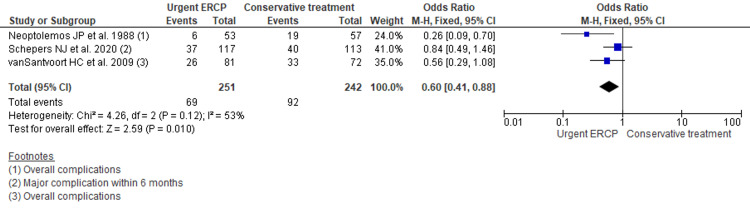
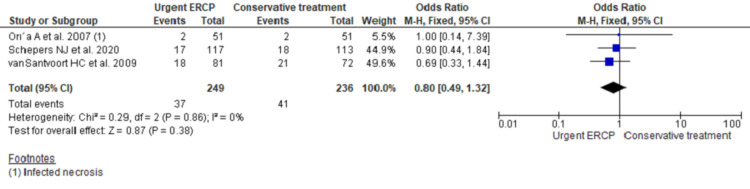
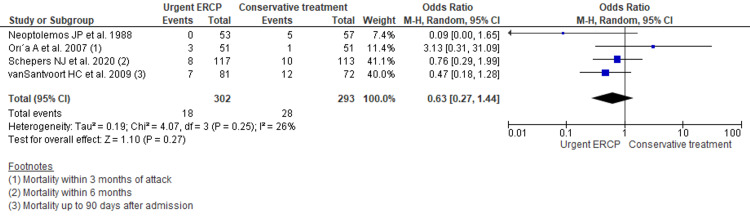
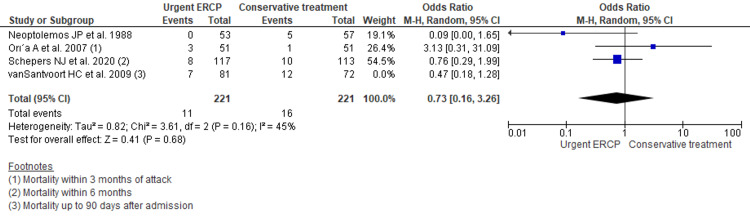
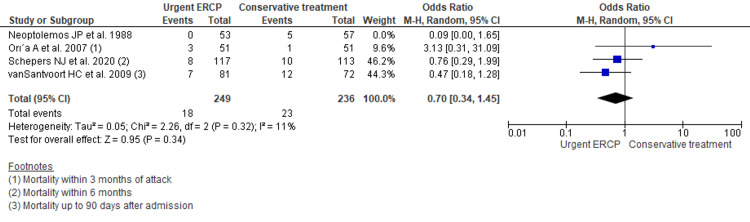
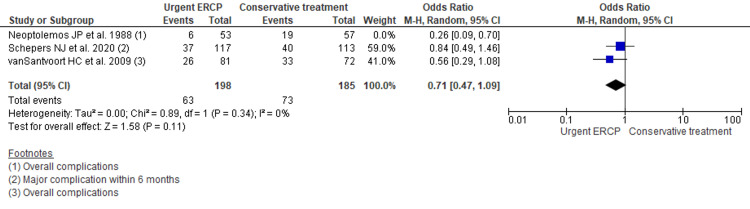
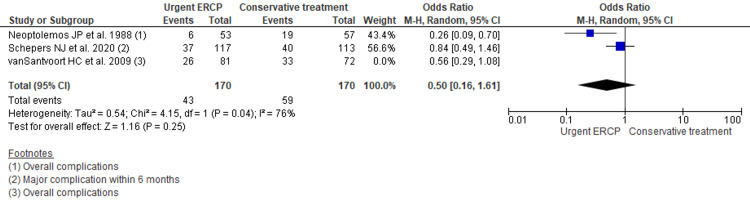
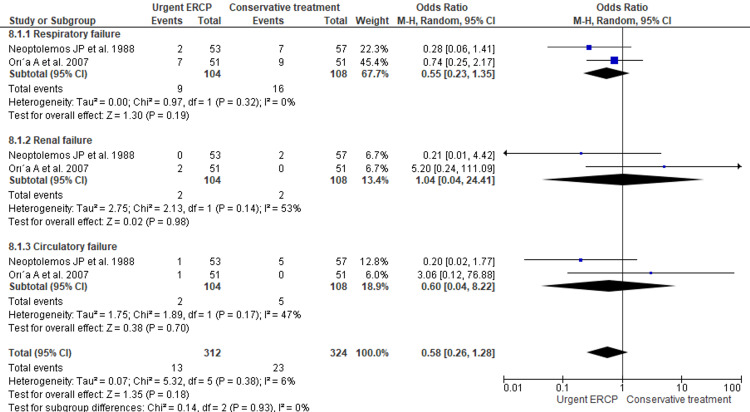
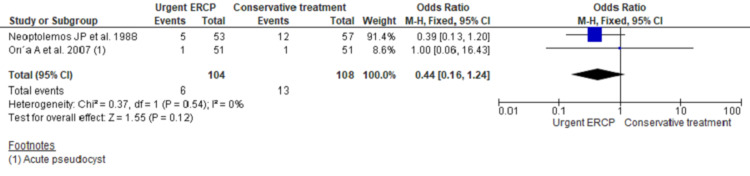
Gallstone disease is the common cause of acute pancreatitis. The role of early endoscopic retrograde cholangiopancreatography (ERCP) in biliary pancreatitis without cholangitis is not well-established. Thus, this study aims to compare the outcome of early ERCP with conservative management in patients with acute biliary pancreatitis without acute cholangitis. An online search of PubMed, PubMed Central, Embase, Scopus, and Clinicaltrials.gov databases was performed for relevant studies published till December 15, 2020. Statistical analysis was performed using RevMan v 5.4 (The Nordic Cochrane Centre, Cochrane Collaboration, Copenhagen). Odds Ratio (OR) with a 95% confidence interval was used for outcome estimation. Among 2700 studies from the database search, we included four studies in the final analysis. Pooling of data showed no significant reduction in mortality (OR 0.59, 95% CI 0.32 to 1.09; p=0.09); overall complications (OR 0.56, 95% CI 0.30 to 1.01; p=0.05); new-onset organ failure (OR 1.06, 95% CI 0.65 to 1.75; p=0.81); pancreatic necrosis (OR 0.80, 95% CI 0.49 to 1.32; p=0.38); pancreatic pseudo-cyst (OR 0.44, 95% CI 0.16 to 1.24; p=0.12); ICU admission (OR 1.64, 95% CI 0.97 to 2.77; p=0.06); and pneumonia development (OR 0.81, 95% CI 0.40 to 1.65; p=0.56) by urgent ERCP comparing with conventional approach for acute biliary pancreatitis without cholangitis. Henceforth, early ERCP in acute biliary pancreatitis without cholangitis did not reduce mortality, complications, and other adverse outcomes compared to the conservative treatment.
Keywords: cholangitis; endoscopic retrograde cholangiopancreatography; meta-analysis; mortality; pancreatitis.
Copyright © 2022, Shrestha et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






Similar articles
-
Urgent endoscopic retrograde cholangiopancreatography with sphincterotomy versus conservative treatment in predicted severe acute gallstone pancreatitis (APEC): a multicentre randomised controlled trial.Lancet. 2020 Jul 18;396(10245):167-176. doi: 10.1016/S0140-6736(20)30539-0. Lancet. 2020. PMID: 32682482 Clinical Trial.
-
Meta-Analysis of Early Endoscopic Retrograde Cholangiopancreatography (ERCP) ± Endoscopic Sphincterotomy (ES) Versus Conservative Management for Gallstone Pancreatitis (GSP).Surg Laparosc Endosc Percutan Tech. 2015 Jun;25(3):185-203. doi: 10.1097/SLE.0000000000000142. Surg Laparosc Endosc Percutan Tech. 2015. PMID: 25799261
-
Early endoscopic retrograde cholangiopancreatography versus conservative management in acute biliary pancreatitis without cholangitis: a meta-analysis of randomized trials.Ann Surg. 2008 Feb;247(2):250-7. doi: 10.1097/SLA.0b013e31815edddd. Ann Surg. 2008. PMID: 18216529 Review.
-
Urgent endoscopic retrograde cholangiopancreatography is not superior to early ERCP in acute biliary pancreatitis with biliary obstruction without cholangitis.PLoS One. 2018 Feb 5;13(2):e0190835. doi: 10.1371/journal.pone.0190835. eCollection 2018. PLoS One. 2018. PMID: 29401491 Free PMC article.
-
Urgent and emergency endoscopic retrograde cholangiopancreatography for gallstone-induced acute cholangitis and pancreatitis.Dig Endosc. 2023 Jan;35(1):47-57. doi: 10.1111/den.14379. Epub 2022 Aug 5. Dig Endosc. 2023. PMID: 35702927 Review.
Cited by
-
Utility of Urgent Endoscopic Retrograde Cholangiopancreatography in Patients with Predicted Mild Acute Pancreatitis and Cholestasis.Dig Dis Sci. 2023 Nov;68(11):4259-4265. doi: 10.1007/s10620-023-08004-1. Epub 2023 Sep 4. Dig Dis Sci. 2023. PMID: 37665426
-
Turkish Society of Gastroenterology: Pancreas Working Group, Acute Pancreatitis Committee Consensus Report.Turk J Gastroenterol. 2024 Nov 11;35(Suppl 1):S1-S44. doi: 10.5152/tjg.2024.24392. Turk J Gastroenterol. 2024. PMID: 39599919 Free PMC article. Review.
-
Exploring the Association Between Paralytic Ileus and Endoscopic Retrograde Cholangiopancreatography Complications Using the National Inpatient Sample Database.Cureus. 2022 Oct 15;14(10):e30319. doi: 10.7759/cureus.30319. eCollection 2022 Oct. Cureus. 2022. PMID: 36407216 Free PMC article.
-
Diagnostic and therapeutic management of severe acute pancreatitis. Evidence based medicine (EBM) clinical practice guidelines.Wideochir Inne Tech Maloinwazyjne. 2025 Apr 9;20(1):1-29. doi: 10.20452/wiitm.2025.17941. eCollection 2025 Apr 9. Wideochir Inne Tech Maloinwazyjne. 2025. PMID: 40547833 Free PMC article. No abstract available.
-
Risk factors for complications in elderly patients aged 85 years and over undergoing endoscopic biliary stone removal.Front Surg. 2022 Oct 11;9:989061. doi: 10.3389/fsurg.2022.989061. eCollection 2022. Front Surg. 2022. PMID: 36303850 Free PMC article.
References
-
- Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta-regression of population-based cohort studies. Xiao AY, Tan MLY, Wu LM, Asrani VM, Windsor JA, Yadav D, Petrov MS. Lanc Gastro Hepa. 2016;1:45–55. - PubMed
-
- Gallstone migration as a cause of acute pancreatitis. Acosta JM, Ledesma CL. N Engl J Med. 1974;290:484–487. - PubMed
-
- Multicentre audit of death from acute pancreatitis. Mann DV, Hershman MJ, Hittinger R, Glazer G. Br J Surg. 1994;81:890–893. - PubMed
Publication types
LinkOut - more resources
Full Text Sources