

Exercise-induced Laryngeal Obstruction: Protocol for a Randomized Controlled Treatment Trial
- PMID: 35198517
- PMCID: PMC8858975
- DOI: 10.3389/fped.2022.817003
Exercise-induced Laryngeal Obstruction: Protocol for a Randomized Controlled Treatment Trial
Abstract
Background: Exercise-induced laryngeal obstruction (EILO) is a common cause of exertional breathing problems in young individuals, caused by paradoxical inspiratory adduction of laryngeal structures, and diagnosed by continuous visualization of the larynx during high-intensity exercise. Empirical data suggest that EILO consists of different subtypes, possibly requiring different therapeutic approaches. Currently applied treatments do not rest on randomized controlled trials, and international guidelines based on good evidence can therefore not be established. This study aims to provide evidence-based information on treatment schemes commonly applied in patients with EILO.
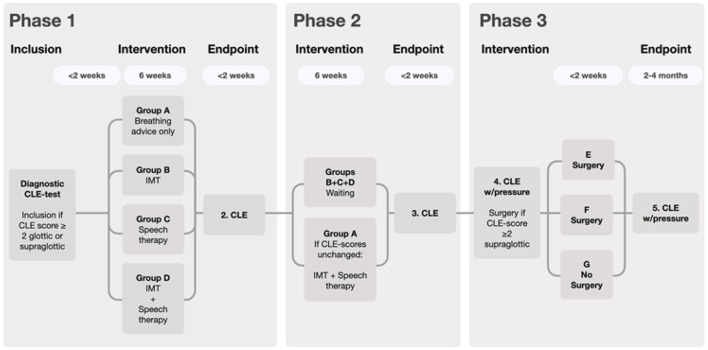
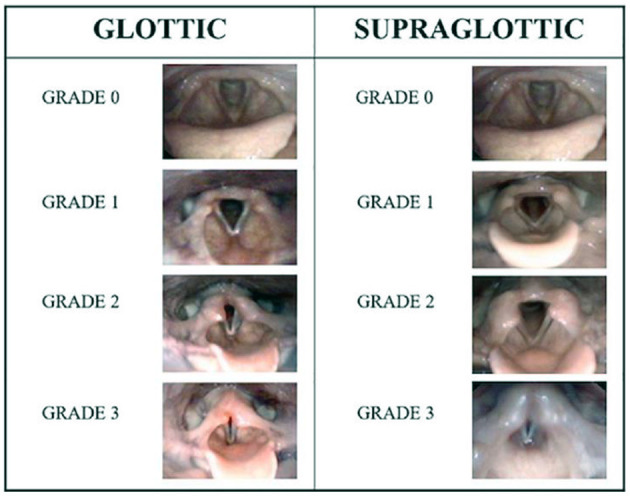
Methods and analysis: Consenting patients consecutively diagnosed with EILO at Haukeland University Hospital will be randomized into four non-invasive treatment arms, based on promising reports from non-randomized studies: (A) standardized information and breathing advice only (IBA), (B) IBA plus inspiratory muscle training, (C) IBA plus speech therapy, and (D) IBA plus inspiratory muscle training and speech therapy. Differential effects in predefined EILO subtypes will be addressed. Patients failing the non-invasive approach and otherwise qualifying for surgical treatment by current department policy will be considered for randomization into (E) standard or (F) minimally invasive laser supraglottoplasty or (G) no surgery. Power calculations are based on the main outcomes, laryngeal adduction during peak exercise, rated by a validated scoring system before and after the interventions.
Ethics and dissemination: The study will assess approaches to EILO treatments that despite widespread use, are insufficiently tested in structured, verifiable, randomized, controlled studies, and is therefore considered ethically sound. The study will provide knowledge listed as a priority in a recent statement issued by the European Respiratory Society, requested by clinicians and researchers engaged in this area, and relevant to 5-7% of young people. Dissemination will occur in peer-reviewed journals, at relevant media platforms and conferences, and by engaging with patient organizations and the healthcare bureaucracy.
Keywords: EILO; RCT (randomized controlled trial); VCD; exercise; protocol; treatment.
Copyright © 2022 Clemm, Røksund, Andersen, Heimdal, Karlsen, Hilland, Fretheim-Kelly, Hufthammer, Sandnes, Hjelle, Vollsæter, Halvorsen and Bergen ILO-group.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer CM declared a shared Committee with one the author J-HH at time of review.
Figures
References
LinkOut - more resources
Full Text Sources